Factors Affecting Learning Curve in Endoscopic Lumbar Discectomy using Interlaminar Approach
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University, College of Medicine, Bucheon, Korea. eungha@unitel.co.kr
Abstract
-
STUDY DESIGN: A retrospective study
OBJECTIVES
To try and find the best surgical technique by analyzing the real-time video taken during a percutaneous endoscopic interlaminar lumbar discectomy. SUMMARY OF LITERATURE REVIEW: A percutaneous endoscopic lumbar discectomy, using an interlaminar approach, has superior aspects, such as anatomical similarity with that of open spinal surgery, and applicability regardless of the herniated level. However, the technical difficulty can be an obstacle to shortening of the learning-curve.
MATERIALS AND METHODS
Between January 2005 and January 2006, 56 patients who were underwent an operation at our hospital, due to single level (L4-5 or L5-S1) herniated lumbar disc disease, by one surgeon, and were selected for this study. The procedure was divided by the approach; either ligament flavum resection, partial removal of the lamina or root identification and discectomy. By analyzing the real-time video taken during the operation, as well as checking the time taken for each procedure, the factors influencing the prolongation of surgery time can be sought, and efforts made to shorten the operation time.
RESULTS
The mean operation time was 65 minutes (28 minutes~127 minutes). The mean operation times in patients either requiring or not requiring partial removal of the lamina were 84 minutes (45 minutes~127 minutes) and 45 minutes (28 minutes~91 minutes), respectively, and also showed a statistically significant correlation (p=0.023). The mean operation times for the first and last 10 cases were 107 and 48 minutes, respectively. 3 cases needed revision open surgery due to failed symptom resolution. The procedures affecting a prolonged operation time were partial removal the lamina and ligament flavum resection. The time required for ligament flavum resection plateaued after 20 cases, and that for partial removal of the lamina reached plateau after 19 cases.
CONCLUSIONS
By overcoming such technical problems, shortening of the learning-curve for a percutaneous endoscopic interlaminar lumbar discectomy was possible.
Figure
-
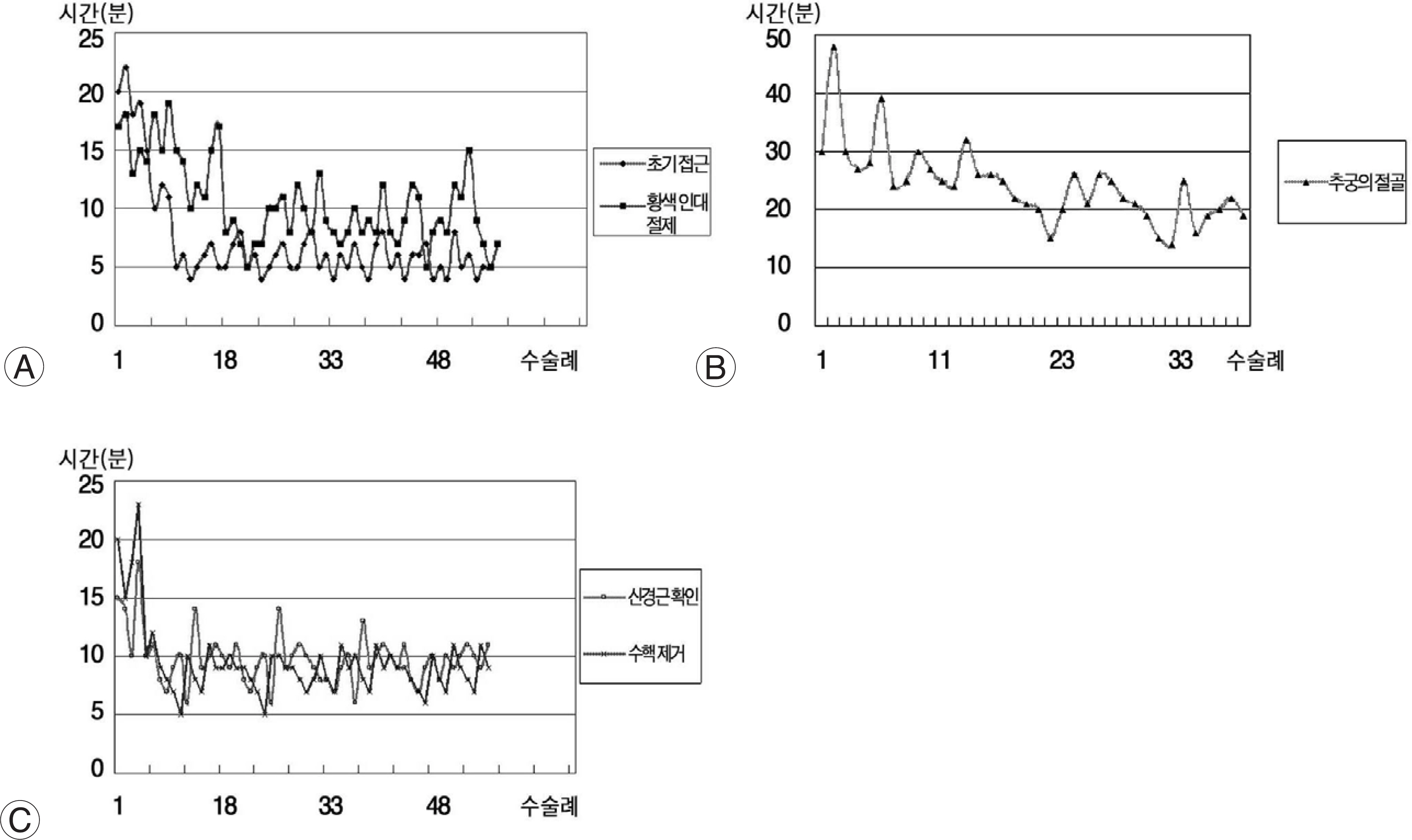
Fig. 1. (A) Lerning curve of initial approach and ligamentum flavum resectioin.(B) Lerning curve of osteotomy. (C) Lerning curve of nerve root identification and herniated disc retraction.
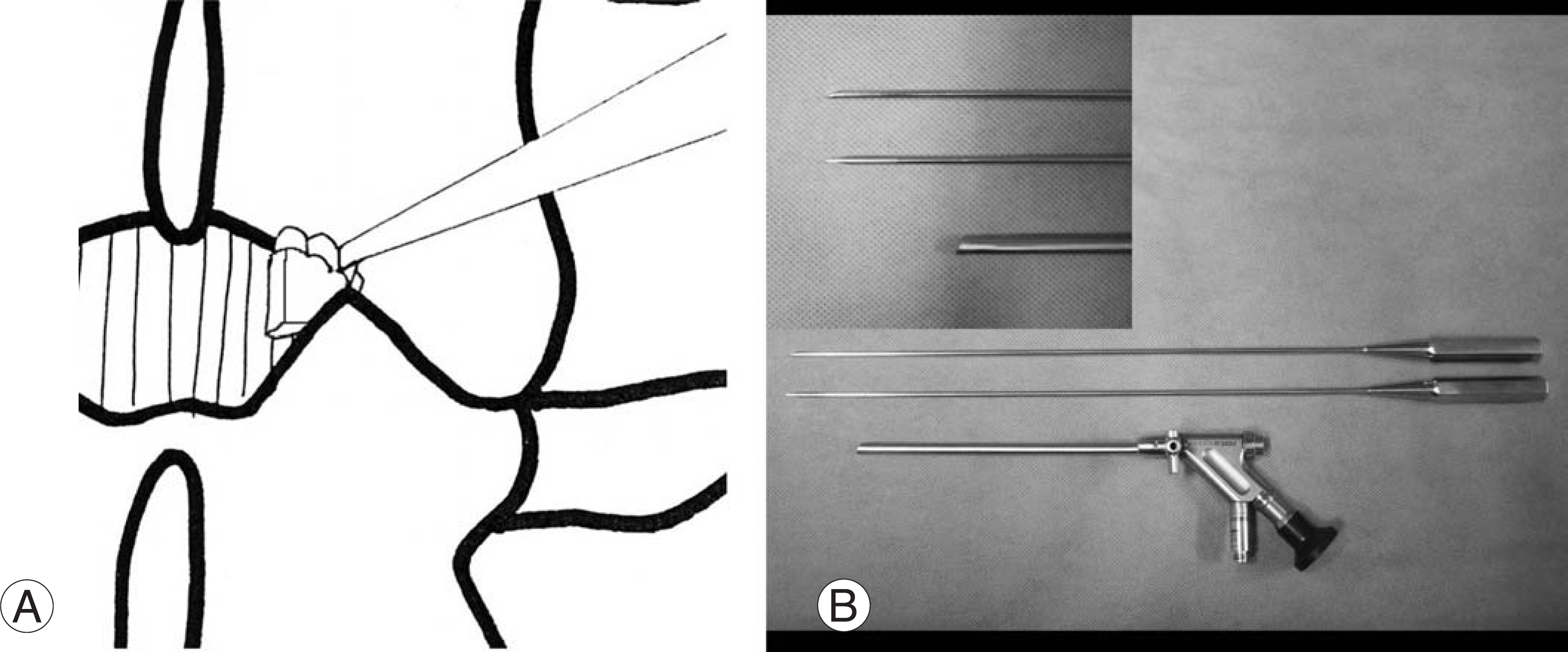
Fig. 2. (A) Using small chisel, lamina on supero-lateral edge of interlaminar space is removed. (B) This photograph shows custom-made 2.5 mm diameter osteotome and chisel.
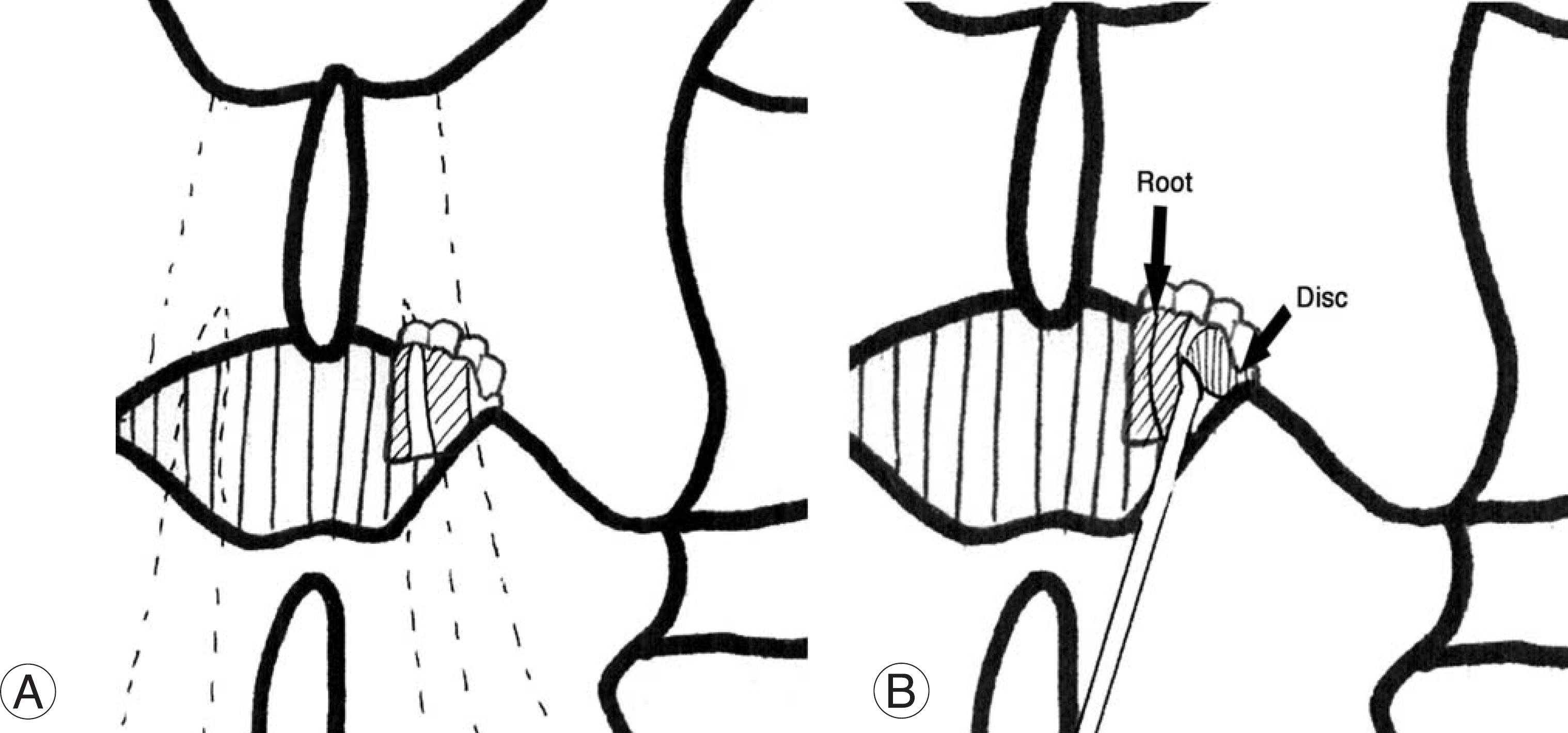
Fig. 3. (A) After resection of ligamentum flavum and osteotomy of lamina, nerve root is exposed. (B) Using probe, nerve root is retracted medially and herniated nucleus is exposed.
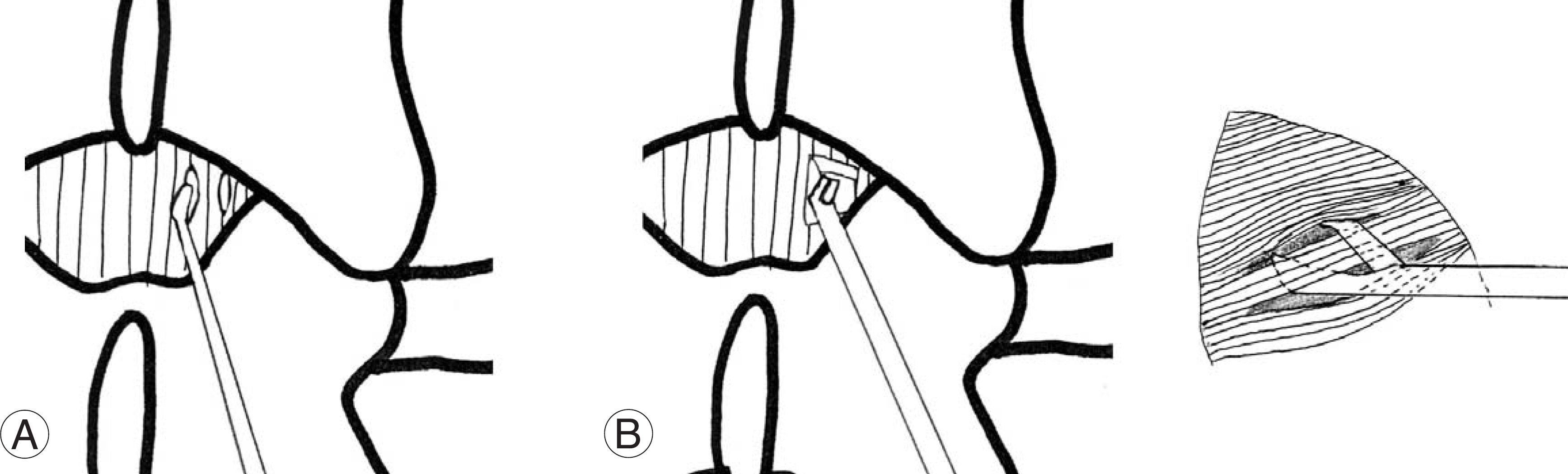
Fig. 4. (A) Small slit is made on the ligamentum flavum using probe. 2 or 3 slits are made for easier resection of ligamentum flavum. (B) Using 2.5mm diameter punch, ligamentum flavum is resected. Punch is introduced through 2 slits and ligamentum flavum between two slits are resected.

Fig. 5. This C-Arm image shows probe located at upper endplate of 5th lumbar vertebrae during operation of L4-5 disc. In which case, there is higher probability of working sheath to be located in axilla of L5 nerve root.
Reference
-
1). Parke WW. The significance of venous return in ischemic radiculopathy and myelopathy. Orthop Clin North Am. 1991; 22:213–220.2). Schick U, Dohnert J, Richter A, et al. Microendoscopic lumbar discectomy versus open surgery: an intraoperative EMG study. Eur Spine J. 2002; 11:20–26.
Article3). Weber BR, Grob D, Dvorak J, et al. .:. Posterior surgical approach to the lumbar spine and its effect on the multi-fidus muscle. Spine. 1997; 22:1765–1772.
Article4). Kambin P. Arthroscopic microdiscectomy. Urban and Scharzenbert, Baltimore. 1991.
Article5). Kambin P, O'Brien E, Zhou L, et al. Arthroscopic mis-codiscectomy and selective fragmentectomy. Clin Orthop. 1998; 347:150–167.6). Kambin P, Sampson S. Posterolateral percutaneous suction-excision of herniated lumbar intervertebral discs: report of interim results. Clin Orthop. 1986; 207:37–43.7). Adson AW, Ott WO. Results of the removal of tumors of the spinal cord. Arch Neurol Psychiatry. 1922; 8:520–538.
Article8). Bucy PC. Chondroma of intervertebral disc. JAMA. 1930; 94:1552.9). Mixter WJ, Barr JS. Rupture of the intervertebral disc with involvement of the spinal canal. N Engl J Med. 1934; 211:205–210.
Article10). Putti V. Pathogenesis of sciatic pain. Lancet. 1927; 53.11). Caspar W. A new surgical procedure for lumbar disc herniation causing less tissue damaging through a microsurgical approach. Adv Neurosurg. 1977; 4:74–77.12). Goald HJ. Microlumbar discectomy: followup of 147 patients. Spine. 1978; 3:183–185.13). Brayda-Bruno M, Cinnella P. Posterior endoscopic discectomy (and other procedures). Eur Spine J. 2000; 9:S24–29.
Article14). Destandau J. A special device for endoscopic surgery of lumbar dsc herniation. Neurol Res. 1999; 21:39–42.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Complications and Management of Endoscopic Spinal Surgery
- Percutaneous Endoscopic Interlaminar Discectomy for L5-S1 Disc Herniation: Axillary Approach and Preliminary Results
- Percutaneous Endoscopic Lumbar Discectomy (PELD) Using Interlaminar Approach in Lumbar Disc Herniation: Endoscopic Laminotomy
- Far Lateral Extraforaminal Disc Herniation after Percutaneous Laser Lumbar Discectomy
- Clinical Results of Interlaminar Approach for Endoscopic Discectomy in the Herniated Lumbar Disc at L5-S1
