Prognostic Factors Affecting the Results of the Surgery for Cervical Spondylotic Myelopathy
- Affiliations
-
- 1Department of Orthopedic Surgery, Asan Medical Center, College of Medicine, Ulsan University, Seoul, Korea. ytkim2@amc.seoul.kr
Abstract
- STUDY DESIGN: This retrospective study was designed to investigate and define the factors affecting the results of surgery for cervical spondylotic myelopathy.
OBJECTIVE
This study was performed in an attempt to investigate and define the factors affecting the results of surgery for cervical spondylotic myelopathy. SUMMARY OF THE LITERATURE REVIEW: There have been few studies about the factors affecting the results of surgery for cervical myelopathy, including MEP (Motor evoked potential) studies and gait analysis, so we investigated the factors that affect the results of surgery for cervical myelopathy.
MATERIALS AND METHODS
We retrospectively studied 59 cervical spondylotic myelopathy patients who underwent operation from Nov. 1994 to Oct. 2002. We analyzed 13 prognostic factors: age, disease duration, the pre-op JOA score, the pre-op. AP canal diameter, the Pavlov ratio, disease level, the AP and lateral cord diameter, the transverse area and the compression ratio at the level of the maximal cord compression on MRI, the cord signal changes on MRI, the MEP(Motor evoked potential) and the gait analysis. The mean follow up period was 29 months. The clinical results were evaluated according to the JOA score. Statistical analysis was performed using the Pearson correlation test, ANOVA and the Kruskal-Wallis test.
RESULTS
The mean pre-op JOA score was 11.1 and the post-op. JOA score was improved to 14.7. The average recovery rate was 67%. The following factors were proved to an influence on the surgical outcomes: age and multiplicity of involvement, and the signal changes of the cord on MRI showed a negative correlation with the recovery rate. The pre-op JOA score, the mean sagittal diameter and the transverse area of the spinal cord at the level of maximum compression showed a positive correlation with the recovery rate. Spasticity on the gait analysis and central conduction block on MEP had an influence on the surgical outcomes.
CONCLUSIONS
The prognostic factors affecting the results of surgery for cervical myelopathy are age, the pre-op JOA score, the disease level, the mean sagittal diameter and the transverse area of the spinal cord at the level of maximum compression, signal change of the cord on MRI, spasticity on the gait analysis and central conduction block on MEP.
MeSH Terms
Figure
-

Fig. 1. Transverse area of the spinal cord.

Fig. 2. Compression ratio = [sagittal diameter (B) / transverse diameter(A)] × 100(%).
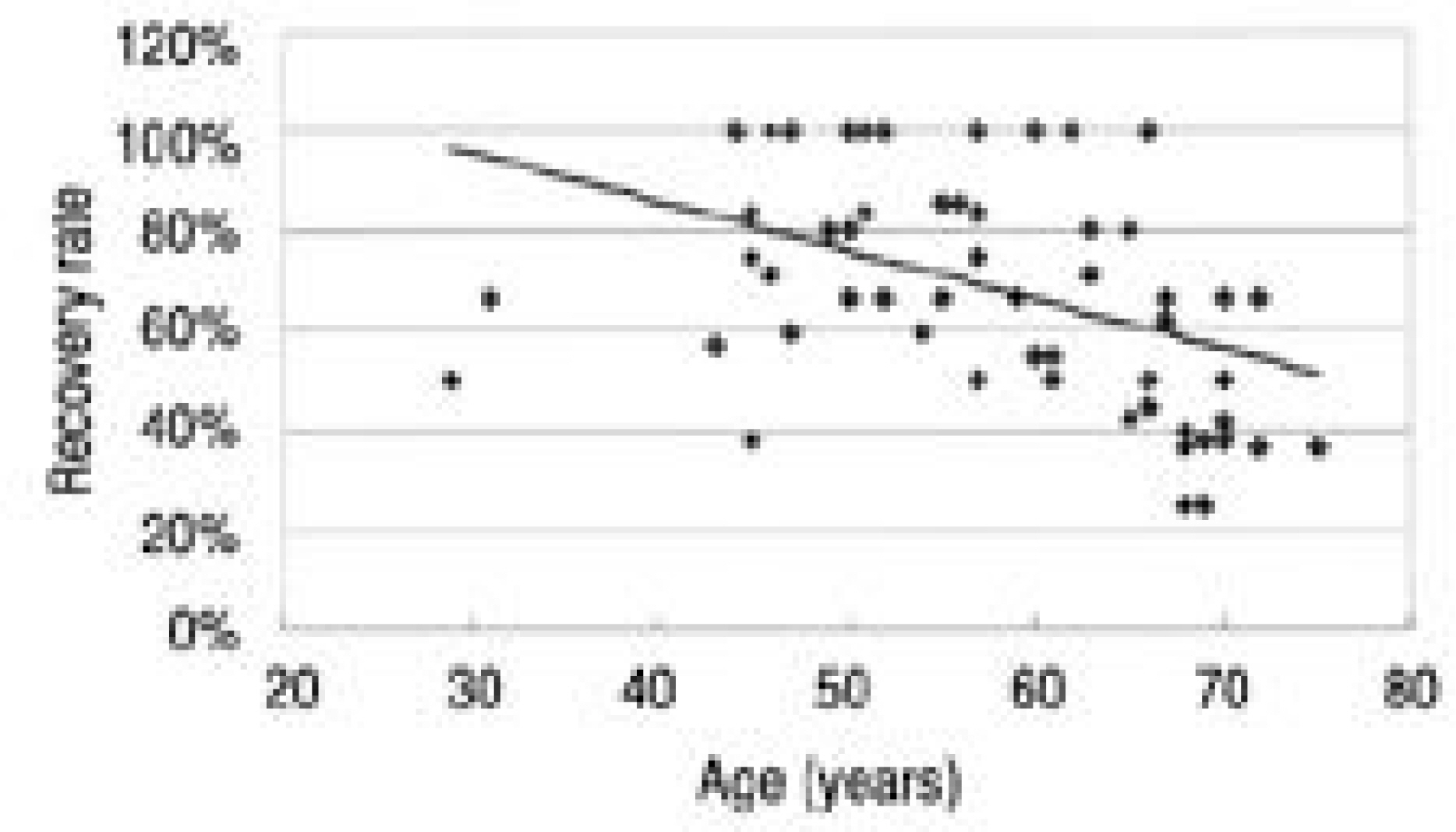
Fig. 3. Correlation between age and recovery rate A negative correlation was observed between age and the recovery rate (r=-0.446, p=0.000).

Fig. 4. Correlation between preoperative JOA score and recovery rate. The preoperative JOA score showed significant correlation with the recovery rate (r=0.683, p=0.000).
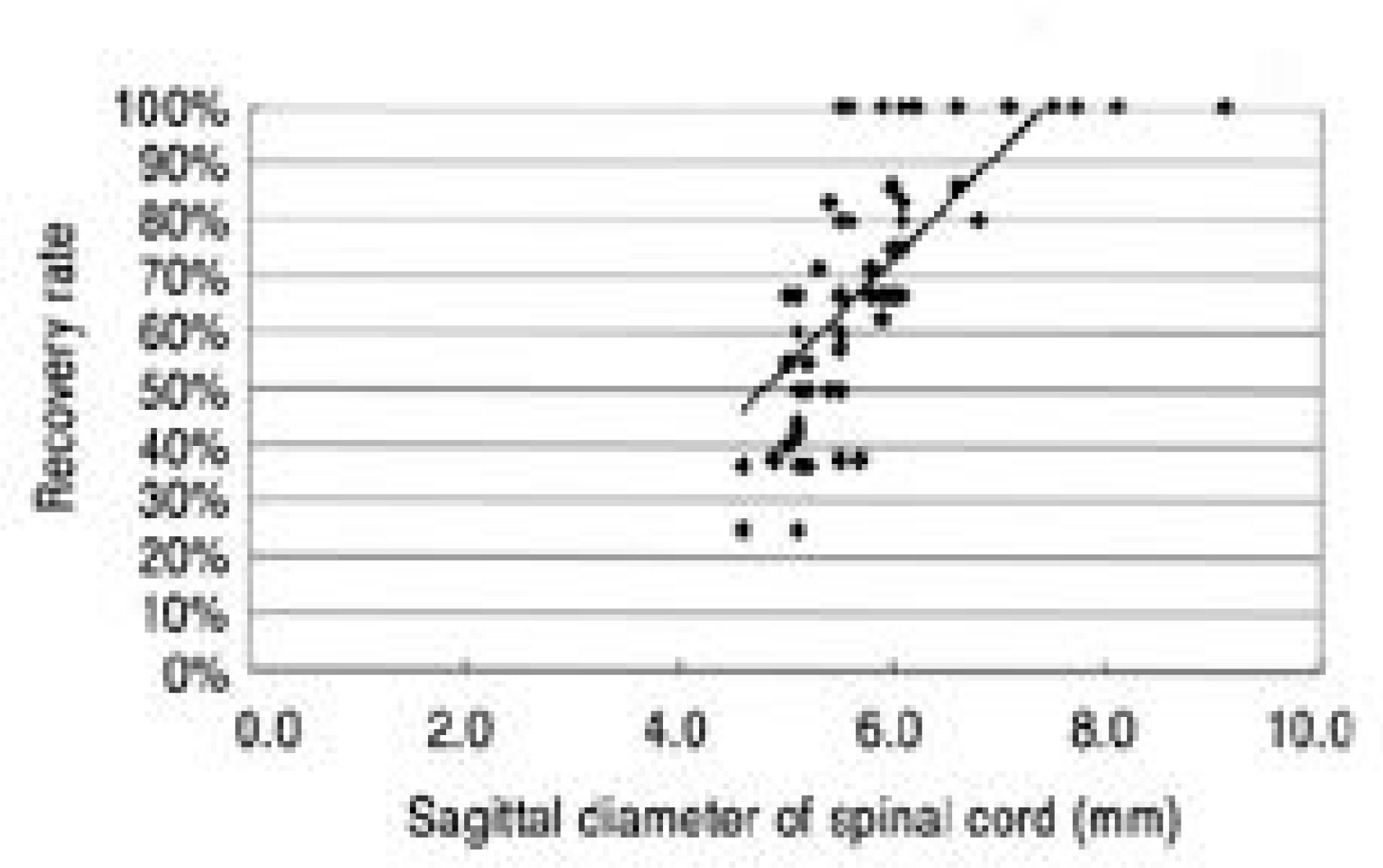
Fig. 5. Correlation between the sagittal diameter of spinal cord and recovery rate. The preoperative sagittal diameter of spinal cord was correlated with the recovery rate (r=0.702, p=0.000).
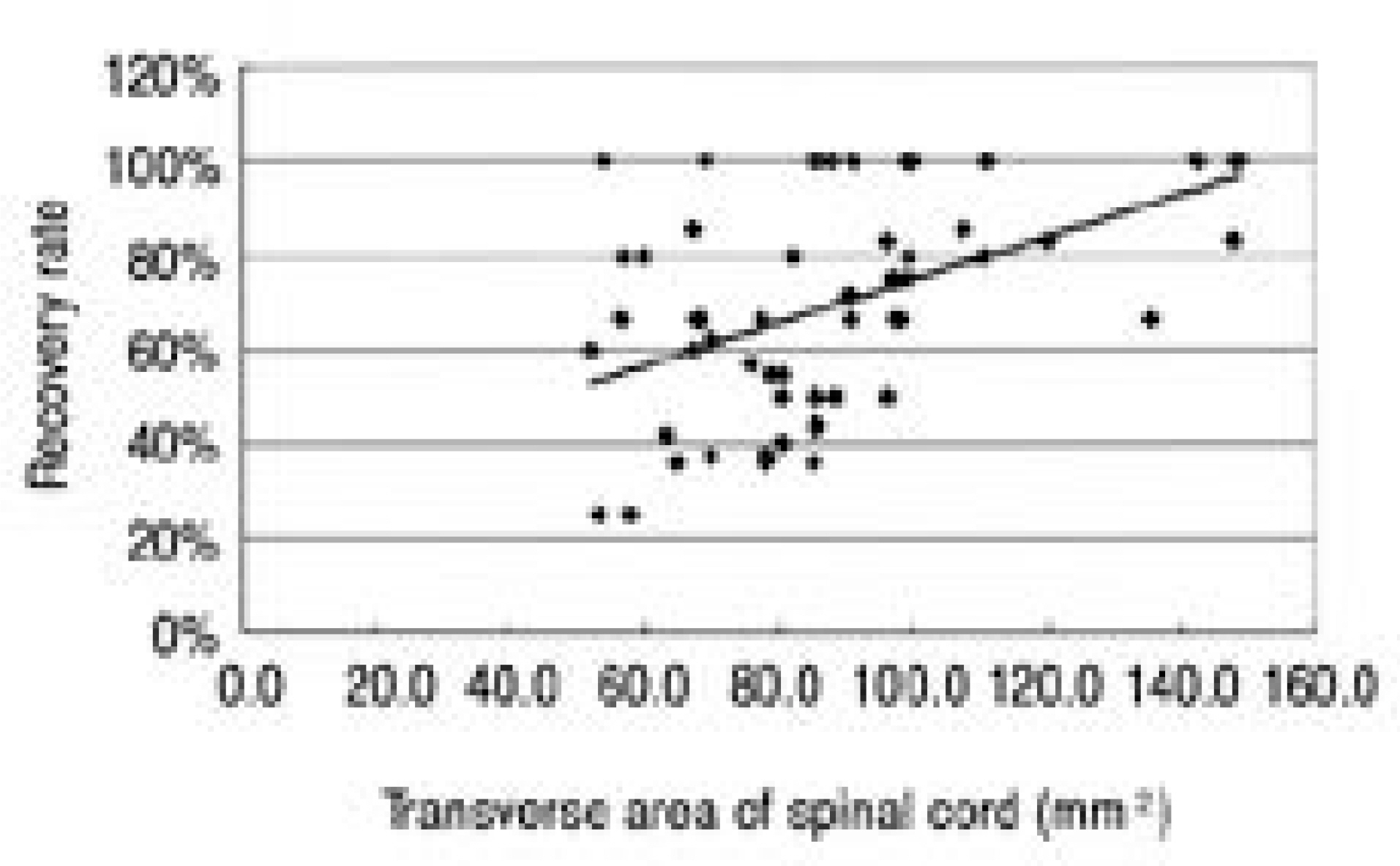
Fig. 6. Correlation between the transverse area of the spinal cord and recovery rate. The preoperative transverse area of the spinal cord showed a positive correlation with the recovery rate (r=0.462 and p=0.000).
Reference
-
1). Fujiwara K, Yonenobu K, Ebara S, Yamashita K, Ono K. The prognosis of surgeryfor cervical compression myelopathy. An analysis of the factors involved. J Bone Joint Surg Br. 1989; 71-B:393–398.2). Kim YT, Lee CS, Yoo JH, Kim TS, Kim JW. Prognostic Factors Affecting the Results of the Surgery for Cervical Myelopathy. J Korean Orthop Assoc. 2004; 39:759–765.
Article3). Lyu RK, Tang LM, Chen CJ, Chen CM, Chang HS, Wu YR. The use of evoked potentials for clinical correlation and surgical outcome in cervical spondylotic myelopathy with intramedullary high signal intensity on MRI. J. Neurol. Neurosurg. Psychiatry. 2004; 75:256–261.4). De Mattei M, Paschero B, Sciarretta A, Davini O, Coc-ito D. Usefulness of motor evoked potentials in compres -sive myelopathy. Electromyogr Clin Neurophysiol. 1993; 33:205–216.5). Goto S, Mochizuki M, Watanabe T, et al. Lon g-term follow-up study of anterior surgery for cervical spondylotic myelopathy with special reference to the magnetic resonance imaging findings in 52 cases. Clin Orthop Rel Res. 291:142–153. 1993.6). Carol MP, Drucker TB. Cervical spondylitic myelopathies: surgical treatment. J Spin Disord. 1988; 1:59–65.7). Kohno K, Kumon Y, Oka Y, Matsui S, Ohue S, Sasaki S. Evaluation of prognostic factors following expansive lamionplasty for cervical spinal stenotic myelopathy. Surg Neurol. 1997; 48:237–245.8). Handa Y, Kubota T, Ishii H, Sato K, Tsuchida A, Arai Y. Evaluation of prognostic factors and clinical outcome in edlerly patients in whom expansive laminoplasty is performed for cervical myelopathy due to multisegmental spongylotic canal stenosis. A retrospective compatison with younger patients. J Neurosurg(Spine2). 2002; 96:173–179.9). Tanaka J, Seki N, Tokimura F, Doi K, Inoue S. Operative results of canal-expansive laminoplasty for cervical spondylotic myelopathy in eldery patients. Spine. 1999; 24:2308–2312.10). Okada Y, Ikata T, Yamada H, Sakamoto R, Katoh S. Magnetic resonance imaging study on the results of surgery for cervical compression myelopathy. Spine. 1993; 18:2024–2029.
Article11). Wada E, Yonenobu K, Suzuki S, Kanazawa A, Ochi T. Can Intramedullary Signal Change on Magnetic Resonance Imaging Predict Surgical Outcome in Cervical Spongylotic Myelopathy? Spine. 1999; 24:455–462.12). Hamburger C, Andreas Buttner A, Uhl E. The Cross-sectional Area of the Cervical Spinal Canal in Patients With Cervical Spondylotic Myelopathy. Spine. 1997; 22:1990–1994.
Article13). Takahashi M, Sakamoto Y, Miyawaki M, Bussaka H. Increased MR signal intensity secondary to cervical cord compression. Neuroradiology. 1987; 29:550–556.14). Morio Y, Yamamoto K, Kuranobu K, Murata M. Does increased signal intensity of the spinal cord in MR images due to cervical myelopathy predict prognosis? Arch Orthop Trauma Surg. 1994; 113:254–259.15). Chang H, Bahk WJ, An JG, Choi KH. Pre and Postoperative Evaluation of Cervical Myelopathy using MR Imaging. J Kor Soc Spine Surg. 1994; 1:326–336.16). Kuhtz-Buschbeck JP, Johnk K, Mader S, Stolze H, Mehdorn M. Analysis of gait in cervical myelopathy. Gait Postur. 1999; 9:184–189.
Article17). Suzuki E, Nakamura H, Konishi S, Yamano Y. Analysis of the Spastic Gait Caused by Cervical Compression Myelopathy. Journal of Spinal Disorders & Techniques. 2002; 15(6):519–522.
Article18). Engsberg JR, Lauryssen C, Ross SA, Hollman JH, Walker D, Wippold FJ 2nd. Spasticity, Strength, and Gait Changes After Surgery for Cervical Spondylotic Myelopathy: A Case Report. Spine. 2003; 28(7):E136–E139.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Factors Affecting Surgical Results in Cervical Spondylotic Myelopathy
- Anterior Cervical Decompression and Fusion for the Treatment of Cervical Spondylotic Myelopathy
- Prognostic Factors Affecting the Surgical Outcome of the Cervical Myelopathy
- Retraction: Sensitivity of Pyramidal Signs in Patients with Cervical Spondylotic Myelopathy
- Vertebral Body Sliding Osteotomy for Cervical Myelopathy With Rigid Kyphosis
