Computed Tomography and Ultrasound of Omental Infarction in Children: Differential Diagnoses of Right Lower Quadrant Pain
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea. hshong@schmc.ac.kr
- 2Department of Radiology, Soonchunhyang University College of Medicine, Cheonan Hospital, Cheonan, Korea.
Abstract
- PURPOSE
Omental infarction in children occurs rarely and is often confused with other diseases that cause right lower quadrant (RLQ) pain. This study evaluates ultrasonography (US) and computed tomography (CT) findings of omental infarction in children with abdominal pain.
MATERIALS AND METHODS
The CT and US findings and clinical presentations of nine children diagnosed with omental infarction between 2005 and 2012 were retrospectively reviewed.
RESULTS
Distributions of abdominal pain in the patients included RLQ (n = 6), right upper quadrant (RUQ, n = 1), periumbilical (n = 1), and the epigastric (n = 1) region. All patients underwent abdominal CT, and three underwent abdominal US. On CT scan, a typical triangular, heterogeneous fatty mass was seen between the abdominal wall and ascending colon (n = 6) or hepatic flexure (n = 1). A fatty mass with an enhanced rim that mimicked acute appendagitis was present in two patients. The other two patients had diffuse fat infiltration without mass. On US, a heterogeneously hyperechoic omental mass was seen in the RLQ (n = 2) or RUQ (n = 1). Three patients underwent appendectomy and partial omentectomy, and pathology confirmed omental infarction.
CONCLUSION
Knowledge of the typical imaging features of omental infarction and application for diagnosis are important for its differentiation from other conditions that also present with RLQ pain and can avoid unnecessary surgery.
MeSH Terms
Figure
-
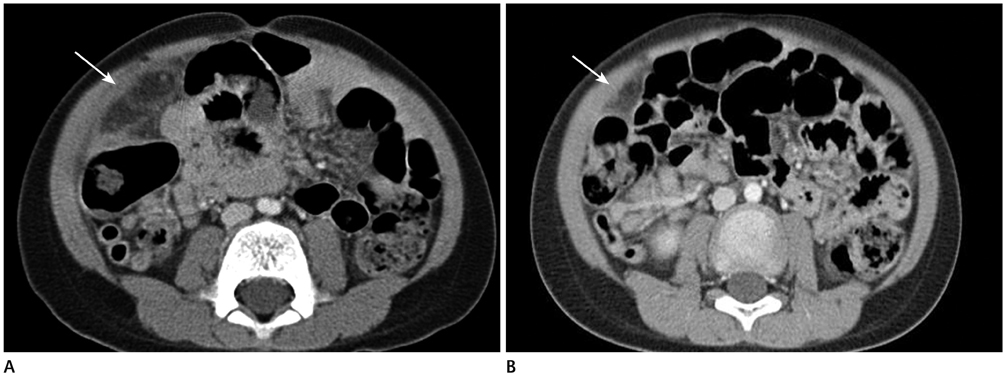
Fig. 1 Postcontrast image from a 4-year-old boy who suffered from RLQ pain for 2 days. A. A triangular-shaped fatty mass (white arrow) is noted between the posterior right lower abdominal wall and the right colon, suggesting omental infarction. B. After 1 month with conservative treatment, follow-up abdominal CT scan was done and decreased in size and enhancement of previously noted fatty mass at RLQ (white arrow). Note.-RLQ = right lower quadrant

Fig. 2 Abdominal ultrasound of a 6-year-old boy with RLQ pain of 2 days' duration. At presentation, ultrasonography (A, B) showed an aggregated hyperechoic fatty mass (white arrow) with increased vascularity. After 1 day, the symptoms had worsened, and follow-up ultrasonography (C, D) showed an aggregated fatty mass with decreased vascularity. The patient underwent laparoscopic omentectomy, which confirmed omental infarction. Note.-RLQ = right lower quadrant
Reference
-
1. Yoo E, Kim JH, Kim MJ, Yu JS, Chung JJ, Yoo HS, et al. Greater and lesser omenta: normal anatomy and pathologic processes. Radiographics. 2007. 27:707–720.2. Chew DK, Holgersen LO, Friedman D. Primary omental torsion in children. J Pediatr Surg. 1995. 30:816–817.3. Helmrath MA, Dorfman SR, Minifee PK, Bloss RS, Brandt ML, DeBakey ME. Right lower quadrant pain in children caused by omental infarction. Am J Surg. 2001. 182:729–732.4. Grattan-Smith JD, Blews DE, Brand T. Omental infarction in pediatric patients: sonographic and CT findings. AJR Am J Roentgenol. 2002. 178:1537–1539.5. Schlesinger AE, Dorfman SR, Braverman RM. Sonographic appearance of omental infarction in children. Pediatr Radiol. 1999. 29:598–601.6. Baldisserotto M, Maffazzoni DR, Dora MD. Omental infarction in children: color Doppler sonography correlated with surgery and pathology findings. AJR Am J Roentgenol. 2005. 184:156–162.7. Nubi A, McBride W, Stringel G. Primary omental infarct: conservative vs operative management in the era of ultrasound, computerized tomography, and laparoscopy. J Pediatr Surg. 2009. 44:953–956.8. Foscolo S, Mandry D, Galloy MA, Champigneulles J, De Miscault G, Claudon M. Segmental omental infarction in childhood: an unusual case of left-sided location with extension into the pelvis. Pediatr Radiol. 2007. 37:575–577.9. Ramos CT, Sammartano R. Laparoscopic omentectomy for omental infarction after bicycle handlebar injury. J Laparoendosc Adv Surg Tech A. 2008. 18:327–329.10. Rimon A, Daneman A, Gerstle JT, Ratnapalan S. Omental infarction in children. J Pediatr. 2009. 155:427–431.e1.11. Aoun N, Nader L, Haddad-Zebouni S, Ghossain M, Akatcherian C. [Left segmental omental infarction in a child: conservative treatment]. Arch Pediatr. 2006. 13:1040–1042.12. Van Kerkhove F, Coenegrachts K, Steyaert L, Ghekiere J, Gabriel C, Casselman JW. Omental infarction in childhood. JBR-BTR. 2006. 89:198–120.13. Yang YL, Huang YH, Tiao MM, Tang KS, Huang FC, Lee SY. Comparison of clinical characteristics and neutrophil values in omental infarction and acute appendicitis in children. Pediatr Neonatol. 2010. 51:155–159.14. Moteki T, Horikoshi H. New CT criterion for acute appendicitis: maximum depth of intraluminal appendiceal fluid. AJR Am J Roentgenol. 2007. 188:1313–1319.15. Singh AK, Gervais DA, Hahn PF, Rhea J, Mueller PR. CT appearance of acute appendagitis. AJR Am J Roentgenol. 2004. 183:1303–1307.16. Ng KS, Tan AG, Chen KK, Wong SK, Tan HM. CT features of primary epiploic appendagitis. Eur J Radiol. 2006. 59:284–288.17. Almeida AT, Melão L, Viamonte B, Cunha R, Pereira JM. Epiploic appendagitis: an entity frequently unknown to clinicians--diagnostic imaging, pitfalls, and look-alikes. AJR Am J Roentgenol. 2009. 193:1243–1251.18. Lucey BC, Stuhlfaut JW, Soto JA. Mesenteric lymph nodes seen at imaging: causes and significance. Radiographics. 2005. 25:351–365.19. Purysko AS, Remer EM, Filho HM, Bittencourt LK, Lima RV, Racy DJ. Beyond appendicitis: common and uncommon gastrointestinal causes of right lower quadrant abdominal pain at multidetector CT. Radiographics. 2011. 31:927–947.20. Alamdaran A, Hiradfar M, Zandi B, Orei M, Taheri R. Diagnostic value of ultrasound findings in mesenteric lymphadenitis in children with acute abdominal pain. Iran J Radiol. 2005. 2:137–140.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Omental Torsion and Infarction with Right Inguinal Hernia: A Case Report
- A Case of Omental Infarct with Right Lower Quadrant Pain
- Omental Infarction Associated with Rib Cage Anomaly in Achondroplasia: Report of a Rare Case
- Idiopathic Omental Infarction to Be a Rare Cause of Acute Abdomen: A Case Report
- A Case of Primary Omental Torsion Presenting as an Acute Abdominal Pain
