Carotid Artery Stenting in Patients with Critical Stenosis of Proximal Internal Carotid Artery and Large Distal Arterial Thrombus: 2 Case Reports
- Affiliations
-
- 1Department of Radiology, Kyung Hee University College of Medicine, Seoul, Korea.
- 2Department of Radiology, Kyung Hee University Hospital, Seoul, Korea. euijkim@hanmail.net
- 3Department of Neurology, Kyung Hee University Hospital, Seoul, Korea.
Abstract
- Determining the timing of carotid artery stenting in patients with carotid artery stenosis with a large territorial infarction is still controversial. Furthermore, it is more difficult to decide the timing of the procedure in cases with a coexisting tandem lesion, including distal arterial stenosis or thrombus. We report two cases of critical stenosis of the proximal internal carotid artery with a coexisting large distal arterial thrombus that presented as a large territorial infarction, that showed resolution of the distal arterial thrombus with stroke management after 3-4 weeks, and that were safely treated with carotid artery stenting.
MeSH Terms
Figure
-
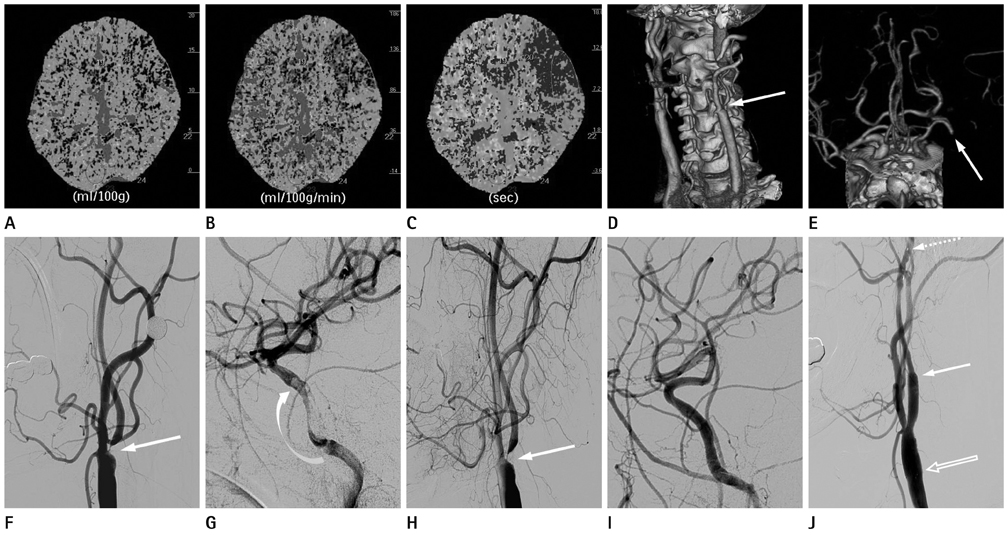
Fig. 1 A 54-year-old man with right side weakness and dysphasia (case 1). A-C. Initial perfusion CT reveals acute infarction at the left frontal lobe, showing decreased CBV (A) and CBF (B), and increased MTT (C). D, E. And initial CT angiography shows severe stenosis of the left proximal internal carotid artery (ICA, arrow in D) and possible occlusion or severe narrowing of the left proximal M1 segment (arrow in E). F, G. Digital subtraction angiography (DSA), obtained 6 days after the initial attack, reveals severe stenosis of the left proximal ICA (arrow in F) and large amount of distal arterial thrombus at the left petrous-cavernous ICA, appearing filling defects (curved arrow in G). H, I. After 4 weeks of 'stroke management' (including dual antiplatelet therapy, lipid lowering therapy, and strict control of the blood pressure), follow-up DSA still shows severe stenosis of the left proximal ICA (arrow in H), however, large amount of filling defects are invisible (I). J. We deploy the stent with the proximal end in the distal common carotid artery (open arrow) and the distal end in the proximal ICA (arrow). DSA also reveals the marker of the protection device (dashed arrow). Note.-CBF = cerebral blood flow, CBV = cerebral blood volume, MTT = mean transit time
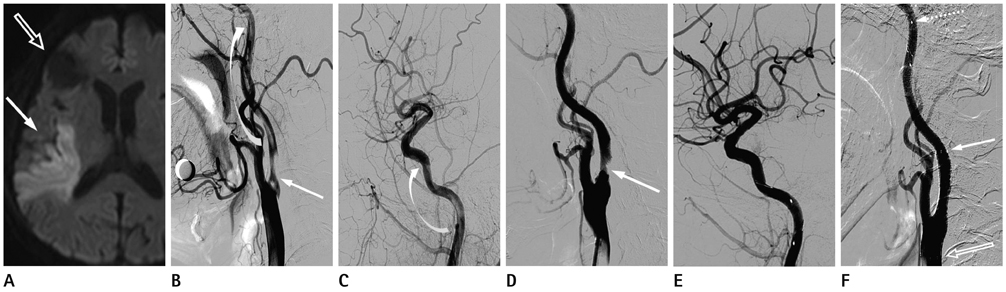
Fig. 2 A 70-year-old man with left side weakness (case 2). A. Initial brain DWI reveals acute focal infarction at the right parietotemporal lobes and right insular cortex (arrow) and chronic focal infarction at the right frontal lobe (open arrow). B, C. DSA shows severe focal stenosis of the right proximal ICA (arrow in B) and reveals large amount of intra-arterial thrombus at right cervical-petrous ICA (curved arrows in B and C). D, E. After 3 weeks of 'stroke management', follow-up DSA reveals no change of severe stenosis of the right proximal ICA (arrow in D), however, reveals no more previous large amount of filling defects at cervical-petrous ICA. F. We deploy the stent with the proximal end in the distal CCA (open arrow) and the distal end in the proximal ICA (arrow). DSA also reveals the marker of the protection device (dashed arrow). Note.-CCA = common carotid artery, DSA = digital subtraction angiography, DWI = diffusion weighted image, ICA = internal carotid artery
Reference
-
1. Jovin TG, Gupta R, Uchino K, Jungreis CA, Wechsler LR, Hammer MD, et al. Emergent stenting of extracranial internal carotid artery occlusion in acute stroke has a high revascularization rate. Stroke. 2005; 36:2426–2430.2. Gasecki AP, Ferguson GG, Eliasziw M, Clagett GP, Fox AJ, Hachinski V, et al. Early endarterectomy for severe carotid artery stenosis after a nondisabling stroke: results from the North American Symptomatic Carotid Endarterectomy Trial. J Vasc Surg. 1994; 20:288–295.3. Paty PS, Darling RC 3rd, Feustel PJ, Bernardini GL, Mehta M, Ozsvath KJ, et al. Early carotid endarterectomy after acute stroke. J Vasc Surg. 2004; 39:148–154.4. Yadav JS, Wholey MH, Kuntz RE, Fayad P, Katzen BT, Mishkel GJ, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004; 351:1493–1501.5. Mantese VA, Timaran CH, Chiu D, Begg RJ, Brott TG. CREST Investigators. The Carotid Revascularization Endarterectomy versus Stenting Trial (CREST): stenting versus carotid endarterectomy for carotid disease. Stroke. 2010; 41:10 Suppl. S31–S34.6. Mathur A, Roubin GS, Iyer SS, Piamsonboon C, Liu MW, Gomez CR, et al. Predictors of stroke complicating carotid artery stenting. Circulation. 1998; 97:1239–1245.7. Roubin GS, Iyer S, Halkin A, Vitek J, Brennan C. Realizing the potential of carotid artery stenting: proposed paradigms for patient selection and procedural technique. Circulation. 2006; 113:2021–2030.8. Delgado MG, Vega P, Mateos V, Bogousslavsky J. Large carotid thrombus. Cerebrovasc Dis. 2009; 27:617–618.9. Yamagami H, Kitagawa K, Ohtsuki T, Matsumoto M, Hori M. Embolic cerebral infarction caused by intraluminal thrombus in the carotid siphon successfully treated with combination of anticoagulant and antiplatelet drugs. Circ J. 2005; 69:1147–1149.10. Kaushansky K, Lichtman M. Williams hematology. 8th ed. China: McGraw Hill;2011. p. 1845–1861.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Transseptal Approach to Carotid Artery Stenting in Right Internal Carotid Stenosis
- Steerable Microcatheter Facilitates Navigation through Tortuous Internal Carotid Artery Lesions in Carotid Artery Stenting
- Carotid Artery Stenting
- Carotid Artery Stenting in a Patient with Spontaneous Recanalization of a Proximal Internal Carotid Artery Occlusion: a Case Report
- Pseudo-no-Reflow Phenomenon in Carotid Artery Stenting using FilterWire EX: Successful Recovery by Aspiration Thrombectomy
