Full-mouth rehabilitation with CAD/CAM monolithic zirconia in dentinogenesis imperfecta: a case report
- Affiliations
-
- 1Department of Prosthodontics and Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Republic of Korea. ksh1250@snu.ac.kr
- 2Department of Dentistry, Ajou University, School of Medicine, Suwon, Republic of Korea.
- KMID: 2321794
- DOI: http://doi.org/10.4047/jkap.2014.52.4.317
Abstract
- Dentinogenesis Imperfecta, with a high incidence rate of 1 : 6 - 8000, is inherited by autosomal dominant genetic transmission. This dental disorder causes discoloration of the teeth and the enamel and dentin show hypoplastic or hypocalcified defects which lead to frequent fractures and rapid attrition. Therefore, timely treatment is necessary for the preservation of the remaining teeth. In this particular case, a 19-year-old patient suffering from Type 1 dentinogenesis imperfecta showed signs of brownish hued teeth with multiple fractures, a loss of vertical dimension, excessive interdental space in the maxillary anterior teeth, and a lack of 5 posterior teeth. To improve the esthetic appearance of the anterior teeth, the vertical dimension was increased. Resin caps were used to alleviate the difficulty of taking an impression of multiple teeth at once. Monolithic zirconia materials used in this case showed high fracture strength and the ability to mask the discoloration of the teeth and therefore, functionally and esthetically favorable results were achieved.
MeSH Terms
Figure
-
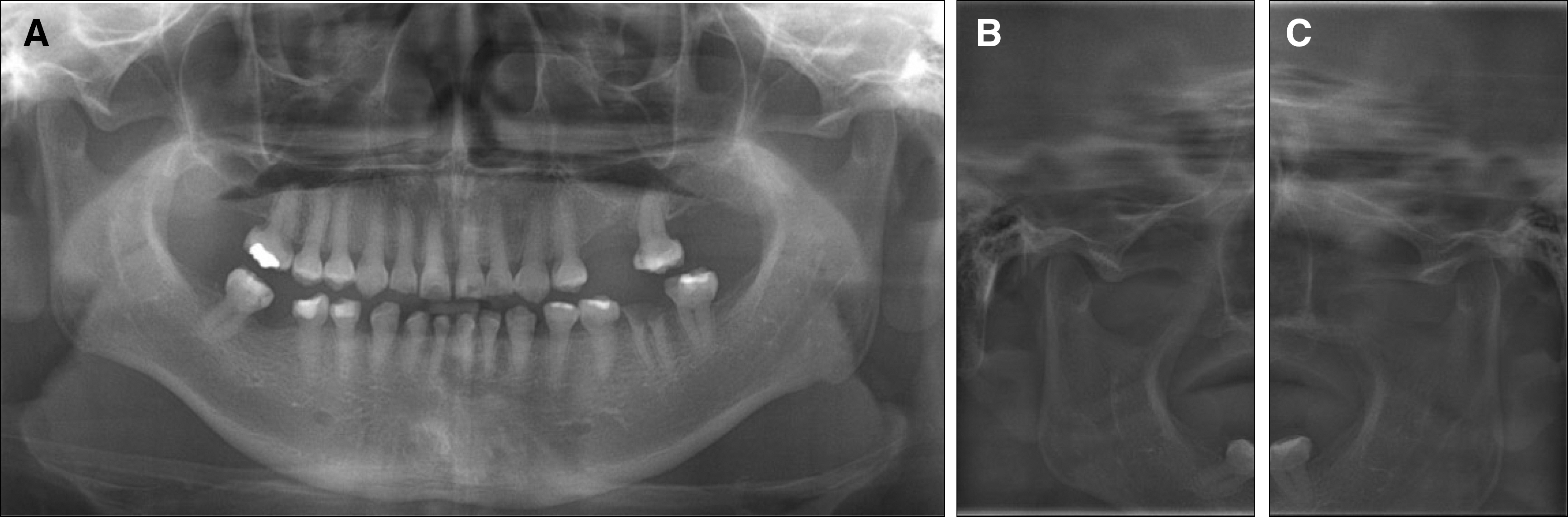
Fig. 1. Initial radiographs of the patient. (A) Panoramic radiograph, (B) Right TMJ panorama, (C) Left TMJ panorama.

Fig. 2. Initial intraoral photographs. (A) Maxillary occlusal view, (B) Frontal view, (C) Mandibular occlusal view.
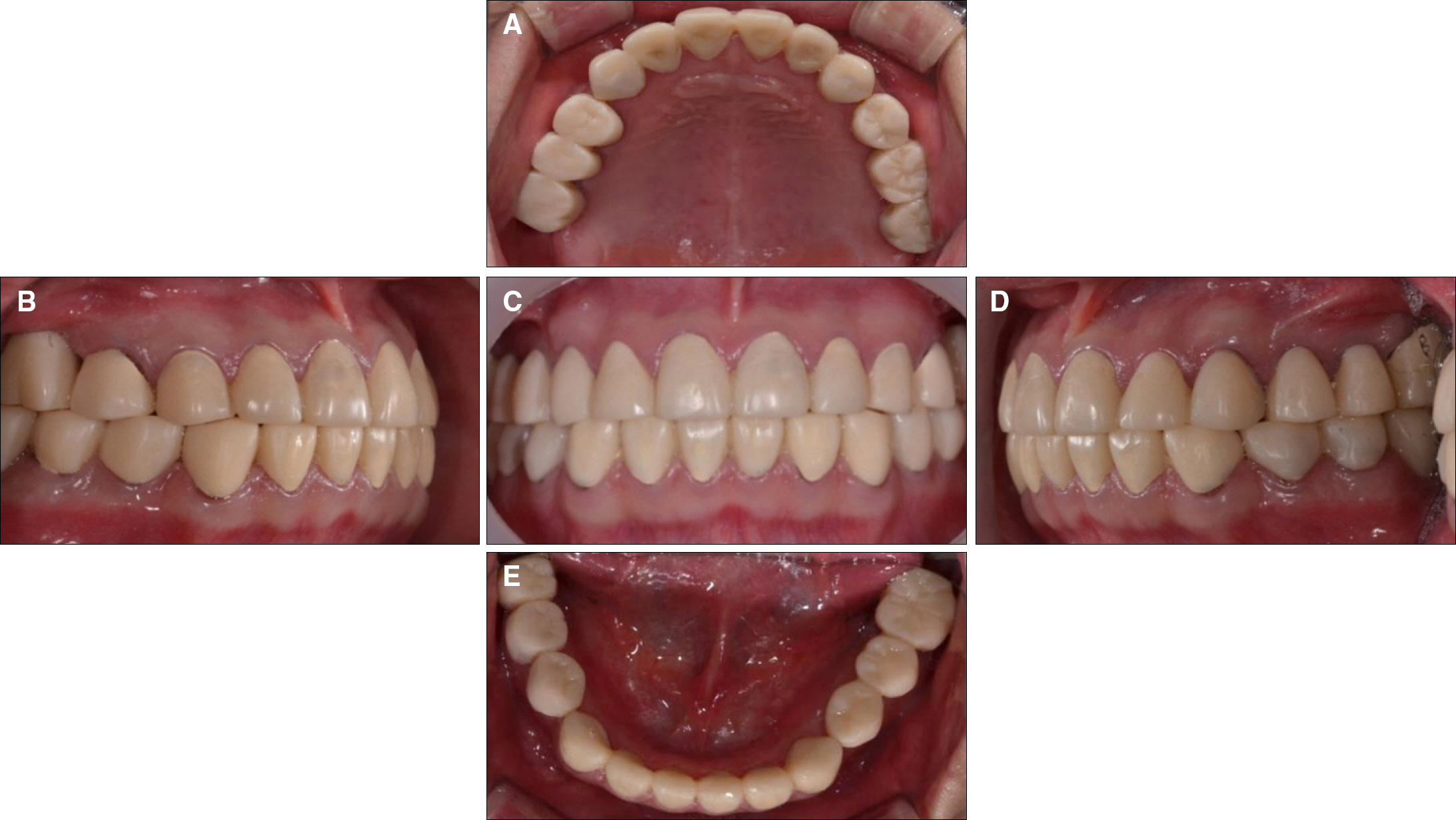
Fig. 3. Provisional Prostheses. (A) Maxillary occlusal view, (B) Lateral view (right), (C) Frontal view, (D) Lateral view (left), (E) Mandibular occlusal view.
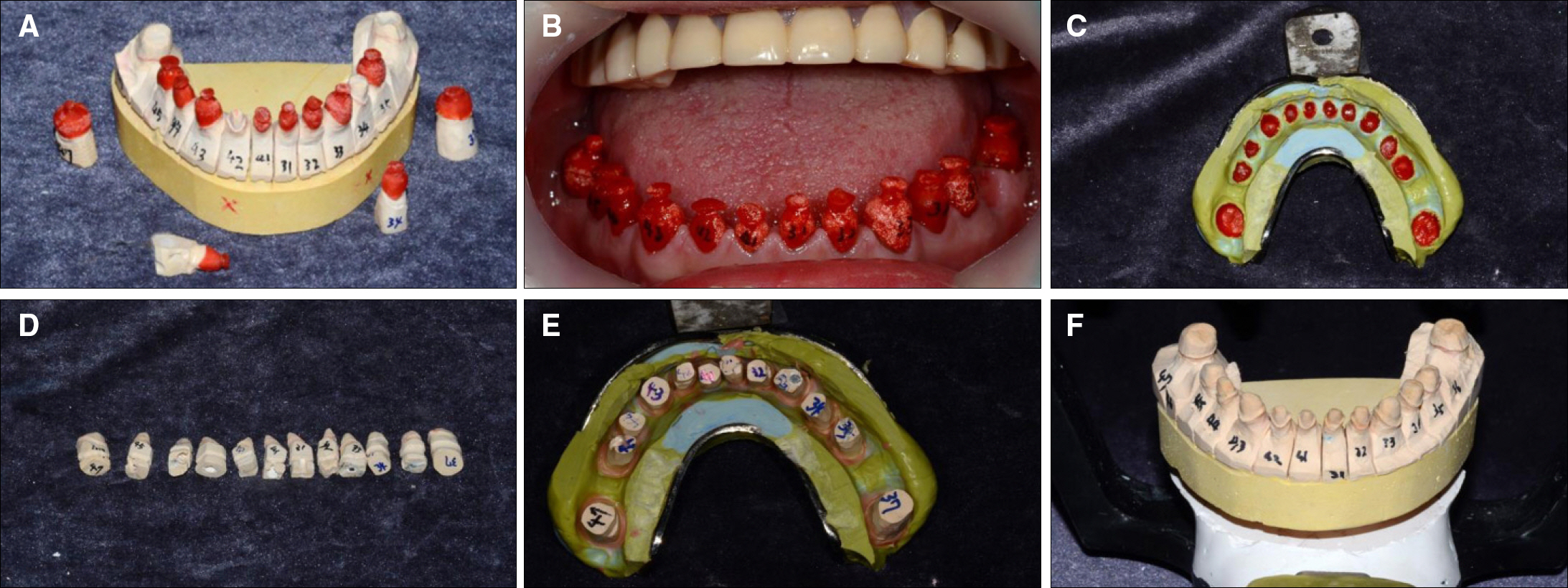
Fig. 4. Pick up impression using Resin caps. (A) Fabrication of the resin caps, (B) Checking for the fitness of the resin caps in oral cavity, (C) Pick-up impression, (D) Separation dies, (E) Positioning of the separation dies into the resin caps, (F) Fabrication of the working cast.
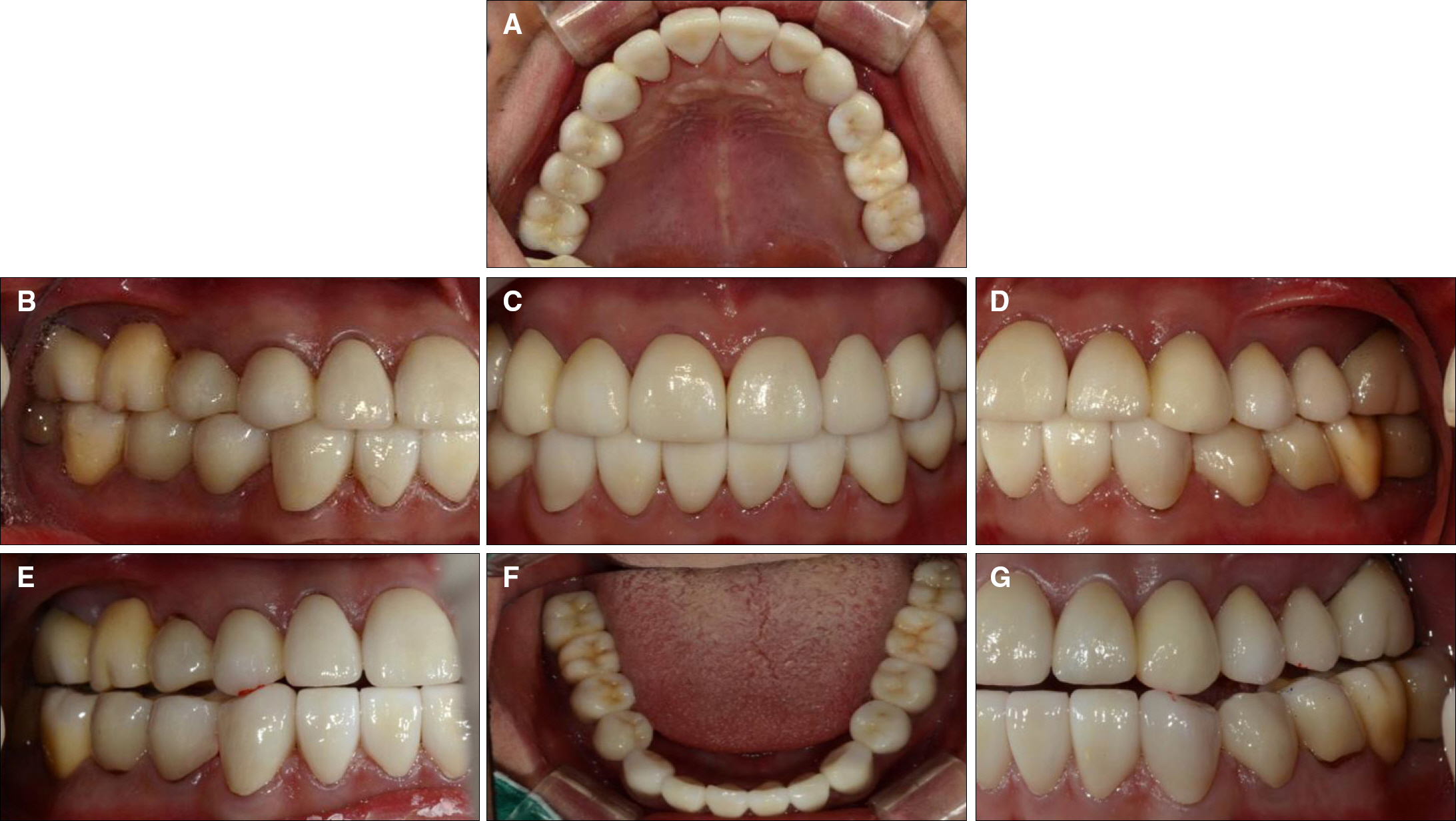
Fig. 5. Intra oral photographs after the placement of definitive prostheses (CAD/CAM monolithic zirconia). (A) Maxillary occlusal view, (B) Lateral view (right), (C) Frontal view, (D) Lateral view (left), (E) Right working movement, (F) Mandibular occlusal view, (G) Left working movement.
Reference
-
1. Witkop CJ Jr. Recent advances in dental genetics. J Dent Res. 1963; 42:1262–75.
Article2. Shields ED, Bixler D, el-Kafrawy AM. A proposed classification for heritable human dentine defects with a description of a new entity. Arch Oral Biol. 1973; 18:543–53.
Article3. O'Connell AC, Marini JC. Evaluation of oral problems in an osteogenesis imperfecta population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:189–96.4. Darendeliler-Kaba A, Mare′chaux SC. Hereditary dentinogenesis imperfecta: a treatment program using an overdenture. ASDC J Dent Child. 1992; 59:273–6.5. Sunderland EP, Smith CJ. The teeth in osteogenesis and dentinogenesis imperfecta. Br Dent J. 1980; 149:287–9.
Article6. Hall RK, Manie′re MC, Palamara J, Hemmerle′ J. Odontoblast dysfunction in osteogenesis imperfecta: an LM, SEM, and ultrastructural study. Connect Tissue Res. 2002; 43:401–5.
Article7. Wieczorek A, Loster J. Dentinogenesis imperfecta type II: ultrastructure of teeth in sagittal sections. Folia Histochem Cytobiol. 2013; 51:244–7.
Article8. Sapir S, Shapira J. Dentinogenesis imperfecta: an early treatment strategy. Pediatr Dent. 2001; 23:232–7.9. Bouvier D, Duprez JP, Morrier JJ, Bois D. Strategies for rehabilitation in the treatment of dentinogenesis imperfecta in a child: a clinical report. J Prosthet Dent. 1996; 75:238–41.
Article10. Henke DA, Fridrich TA, Aquilino SA. Occlusal rehabilitation of a patient with dentinogenesis imperfecta: a clinical report. J Prosthet Dent. 1999; 81:503–6.
Article11. Bouvier D, Leheis B, Duprez JP, Bittar E, Coudert JL. Dentinogenesis imperfecta: long-term rehabilitation in a child. J Dent Child (Chic). 2008; 75:192–6.12. Rivera-Morales WC, Mohl ND. Relationship of occlusal vertical dimension to the health of the masticatory system. J Prosthet Dent. 1991; 65:547–53.
Article13. Smith BH. Changes in occlusal face height with removable partial prostheses. J Prosthet Dent. 1975; 34:278–85.
Article14. Moundouri-Andritsakis H, Kourtis SG, Andritsakis DP. All-ce-ramic restorations for complete-mouth rehabilitation in dentinogenesis imperfecta: a case report. Quintessence Int. 2002; 33:656–60.15. American Academy on Pediatric Dentistry Council on Clinical Affairs. Guideline on oral heath care/dental management of heritable dental development anomalies. Pediatr Dent. 2008-2009; 30:196–201.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full mouth rehabilitation of a patient using monolithic zirconia and dental CAD/CAM system: a case report
- Full mouth rehabilitation using monolithic zirconia: a clinical report
- Maxillary cement retained implant supported monolithic zirconia prosthesis in a full mouth rehabilitation: a clinical report
- Full-mouth rehabilitation in an amelogenesis imperfecta patient with anterior open bite using CAD/CAM system
- A full-mouth rehabilitation using zirconia all-ceramic crowns: a case report
