Spontaneous Splenic Rupture as a Paradoxical Reaction during Treatment for Splenic Tuberculosis
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea. sooli10kr@yahoo.co.kr
- 2Department of Pathology, Pusan National University Yangsan Hospital, Pusan National University School of Medicine, Yangsan, Korea.
Abstract
- This report describes a rare case of a patient with splenic tuberculosis (TB) who developed spontaneous splenic rupture after 10 weeks of antituberculous chemotherapy. The patient responded well to the antituberculous regimen prior to the spontaneous splenic rupture. We considered a paradoxical reaction as a cause of the splenic rupture. The patient underwent splenectomy and continuously received initial antituberculous drugs without change. To the best of our knowledge, this is the first report of spontaneous splenic rupture as a paradoxical reaction to antituberculous chemotherapy in an immunocompetent host with splenic TB.
MeSH Terms
Figure
-
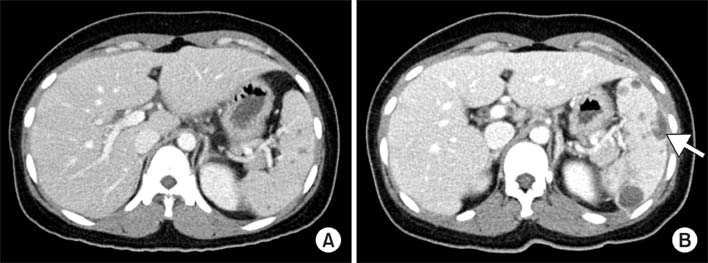
Figure 1 Computed tomography (CT) findings of the abdomen. (A) Initial CT shows multiple hypodense lesions in the spleen. (B) After 10 weeks of chemotherapy, CT shows more increase in the size and number of splenic abscesses with intraperitoneal rupture (arrow).
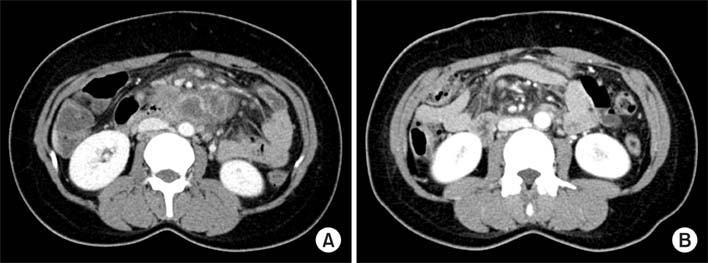
Figure 2 Computed tomography (CT) findings of the abdomen. (A) Initial CT shows several central low density with peripheral rim enhanced lymph nodes enlargement around small bowel mesentery. (B) After 10 weeks of chemotherapy, CT shows decreased interval in the size and number of those lymph node lesions.
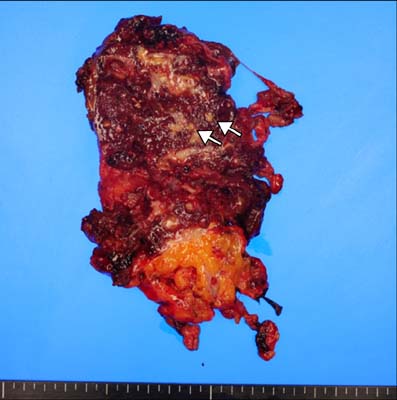
Figure 3 Explanted spleen. By gross appearance, the spleen was enlarged, measuring approximately 14×9×4 cm in dimension and 232.8 g in weight. The specimen shows multiple yellow necrotic nodules (arrows) and foci of hemorrhage.

Figure 4 Histopathological findings of the spleen. (A) Large granuloma with central necrosis is noted (H&E stain, ×40). (B) Epithelioid and Langhans giant cells (box: arrow) are identified at the peripheral portion of the granuloma (H&E stain, ×100).
Reference
-
1. Peto HM, Pratt RH, Harrington TA, LoBue PA, Armstrong LR. Epidemiology of extrapulmonary tuberculosis in the United States, 1993-2006. Clin Infect Dis. 2009; 49:1350–1357.2. Sharma SK, Smith-Rohrberg D, Tahir M, Mohan A, Seith A. Radiological manifestations of splenic tuberculosis: a 23-patient case series from India. Indian J Med Res. 2007; 125:669–678.3. Pramesh CS, Tamhankar AP, Rege SA, Shah SR. Splenic tuberculosis and HIV-1 infection. Lancet. 2002; 359:353.4. Rathore S, George P, Deodhar M, Calton N, George U, Pawar B, et al. Spontaneous rupture of tuberculous spleen in a HIV seropositive patient on maintenance hemodialysis. Saudi J Kidney Dis Transpl. 2009; 20:822–825.5. Lam KY, Ng WF, Chan AC. Miliary tuberculosis with splenic rupture: a fatal case with hemophagocytic syndrome and possible association with long standing sarcoidosis. Pathology. 1994; 26:493–496.6. Ram R, Swarnalatha G, Prasad N, Murty KV. Pathological rupture of spleen in a haemodialysis patient due to tuberculosis. Nephrol Dial Transplant. 2006; 21:2994–2995.7. Weber E, Gunthard HF, Schertler T, Seebach JD. Spontaneous splenic rupture as manifestation of the immune reconstitution inflammatory syndrome in an HIV type 1 infected patient with tuberculosis. Infection. 2009; 37:163–165.8. Rao RC, Ghose R, Sawhney S, Berry M. Hemangioma of spleen with spontaneous, extra-peritoneal rupture, with associated splenic tuberculosis: an unusual presentation. Australas Radiol. 1993; 37:100–101.9. Safioleas MC, Stamatakos MC, Safioleas CM, Diab AI, Agapitos EB. Co-existence of spontaneous splenic rupture and tuberculosis of the spleen. Saudi Med J. 2006; 27:1588–1590.10. Fegan D, Butcher C, Rees C, Glennon J. Tuberculosis and abdominal pain. Intern Med J. 2005; 35:437–438.11. Sterlacci W, Heiss S, Augustin F, Tzankov A. Splenic rupture, beyond and behind: a histological, morphometric and follow-up study of 254 cases. Pathobiology. 2006; 73:280–287.12. Renzulli P, Hostettler A, Schoepfer AM, Gloor B, Candinas D. Systematic review of atraumatic splenic rupture. Br J Surg. 2009; 96:1114–1121.13. Breen RA, Smith CJ, Bettinson H, Dart S, Bannister B, Johnson MA, et al. Paradoxical reactions during tuberculosis treatment in patients with and without HIV co-infection. Thorax. 2004; 59:704–707.14. Carvalho AC, De Iaco G, Saleri N, Pini A, Capone S, Manfrin M, et al. Paradoxical reaction during tuberculosis treatment in HIV-seronegative patients. Clin Infect Dis. 2006; 42:893–895.15. Park KY, Lee HJ, Jung JW, Choi YH, Nam SB, Ahn SH, et al. A case of different response of miliary lung and intracranial nodules to antituberculous therapy. Tuberc Respir Dis. 2008; 64:153–157.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Splenic Rupture
- Spontaneous Rupture of Primary Angiosarcoma of the Spleen
- A case of splenic artery aneurysm rupture complicated by liver cirrhosis
- Atraumatic Splenic Hemorrhage as a Rare Complication of Pancreatitis: Case Report and Literature Review
- A Case of Spontaneous Splenic Rupture in Vivax Malaria
