Successful Embolization in the Patient with Hemoptysis Due to Right Inferior Phrenic Artery-pulmonary Artery Anastomosis and Pseudoaneurysm
- Affiliations
-
- 1Division of Pulmonology, Konyang University College of Medicine, Daejon, Korea. sjoongkwon@hanmail.net
- 2Department of Diagnostic Radiology, Konyang University College of Medicine, Daejon, Korea.
Abstract
- The primary cause of hemoptysis is the bronchial artery. However, it should be noted that pulmonary artery and other vessels can cause hemoptysis. If the source of the bleeding is not determined after embolization, other evaluations are needed. Systemic-pulmonary anastomosis and pulmonary artery pseudo-aneurysm are rare vascular abnormalities with varying etiologies. An accurate and rapid diagnosis is needed in hemoptysis, since the cause may be life-threatening. We report a case of a 77-years-old man with persistent hemoptysis due to the right inferior phrenic artery - pulmonary artery anastomosis and pseudoaneurysm. After the embolization of the inferior phrenic artery, the hemoptysis was successfully treated.
Keyword
Figure
-
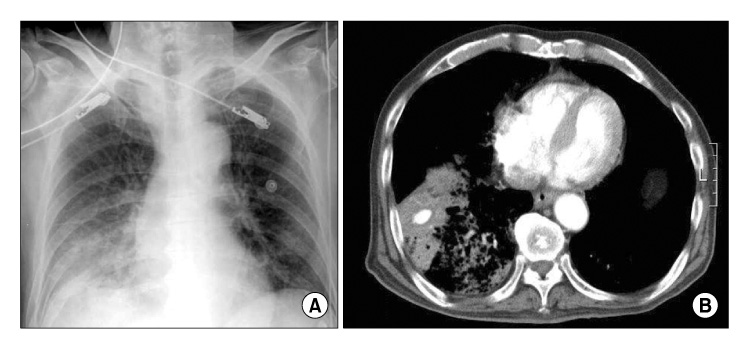
Figure 1 (A) Initial chest X-ray at admission shows haziness in right lower lung. (B) Chest CT scan shows consolidation and ground glass opacity with 1.5 cm size, well marginated enhancing nodule in right lower lung.
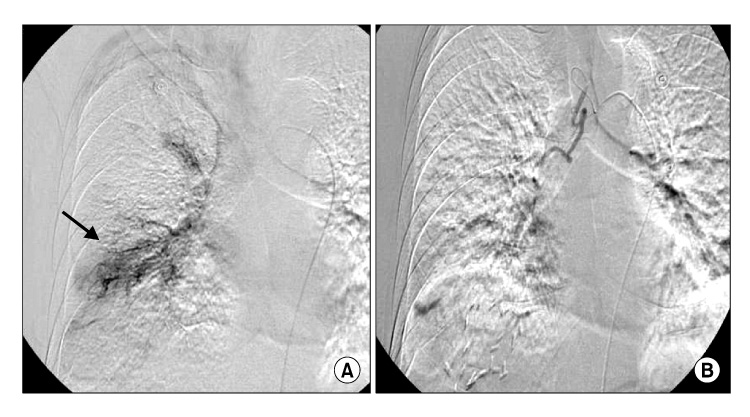
Figure 2 (A) Right bronchial angiogram, active bleeding (arrow) from branch of right lower bronchial artery are shown. (B) Bronchial artery embolization was done using the contour particle.
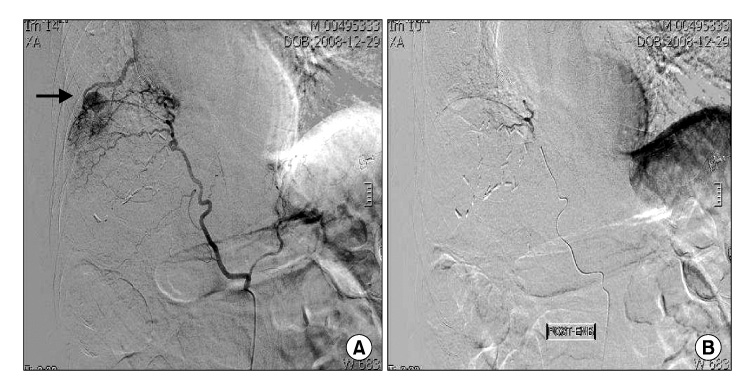
Figure 3 (A) Inferior phrenic angiogram shows a pseudoaneurysm arising (arrow) from the right inferior phrenic artery shunting to right pulmonary artery. (B) After embolization with contour particle at distal part of right inferior phrenic artery, there was no more bleeding.
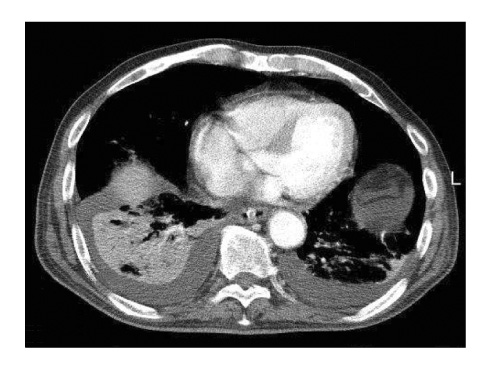
Figure 4 Disappeared pseudoaneurysm of right lower lobe in chest CT scan at 10 days after embolization.
Reference
-
1. Remy-Jardin M, Remy J. Spiral CT angiography of the pulmonary circulation. Radiology. 1999. 212:615–636.2. Fraser RS, Muller NL, Colman N, Pare PD. Fraser RS, Muller NL, Colman N, Pare PD, editors. Pulmonary hypertension and edema. Diagnosis of disease of the chest. 1999. Philadelphia: Saunders;1935–1937.3. Webb WR, Jacobs RP. Transpleural abdominal systemic artery-pulmonary artery anastomosis in patients with chronic pulmonary infection. AJR Am J Roentgenol. 1977. 129:233–236.4. Chung JW, Park JH, Han JK, Choi BI, Kim TK, Han MC. Transcatheter oily chemoembolization of the inferior phrenic artery in hepatocellular carcinoma: the safety and potential therapeutic role. J Vasc Interv Radiol. 1998. 9:495–500.5. Takanami I. Massive haemoptysis due to chronic pancreatitis: control with inferior phrenic artery embolization. Eur J Cardiothorac Surg. 2000. 18:120–122.6. Khalil A, Fartoukh M, Tassart M, Parrot A, Marsault C, Carette MF. Role of MDCT in identification of the bleeding site and the vessels causing hemoptysis. AJR Am J Roentgenol. 2007. 188:117–125.7. Shigemura N, Wan IY, Yu SC, Wong RH, Hsin MK, Thung HK, et al. Multidisciplinary management of life-threatening massive hemoptysis: a 10-year experience. Ann Thorac Surg. 2009. 87:849–853.8. Chun HJ, Byun JY, Yoo SS, Choi BG. Added benefit of thoracic aortography after transarterial embolization in patients with hemoptysis. AJR Am J Roentgenol. 2003. 180:1577–1581.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Thrombin Injection for a Pulmonary Artery Pseudoaneurysm: Case Report
- A Case of Pulmonary Artery Pseudoaneurysm Treated by Embolization
- Percutaneous Transhepatic Venous Embolization of Pulmonary Artery Aneurysm in Hughes - Stovin Syndrome
- Coronary to Bronchial Artery Fistula Causing Massive Hemoptysis in Patients with Longstanding Pulmonary Tuberculosis
- A Case of Pseudoaneurysm Due to Fungus Ball within the Progressive Massive Fibrosis in a Patient with Pneumoconiosis: Computed Tomography-Pathologic Correlation
