Coronary to Bronchial Artery Fistula Causing Massive Hemoptysis in Patients with Longstanding Pulmonary Tuberculosis
- Affiliations
-
- 1Department of Radiology, Hallym University College of Medicine, Gyeonggi-do 431-070, Korea. jeyrad@hanmail.net
- KMID: 1058801
- DOI: http://doi.org/10.3348/kjr.2012.13.1.102
Abstract
- We report on three cases of longstanding pulmonary tuberculosis patients with coronary to bronchial artery fistula (CBF) who presented with recurrent massive hemoptysis. The first and second patients died because of decreased functional pulmonary volume plus massive hemoptysis and cannulation failure of CBF due to hypovolemic vasospasm, respectively. When recurrent hemoptysis occurs despite successful embolization treatment, CBF should be considered as a potential bleeding source. Moreover, a coronary angiography should be performed, especially in patients with longstanding cardiopulmonary disease such as pulmonary tuberculosis.
MeSH Terms
Figure
-
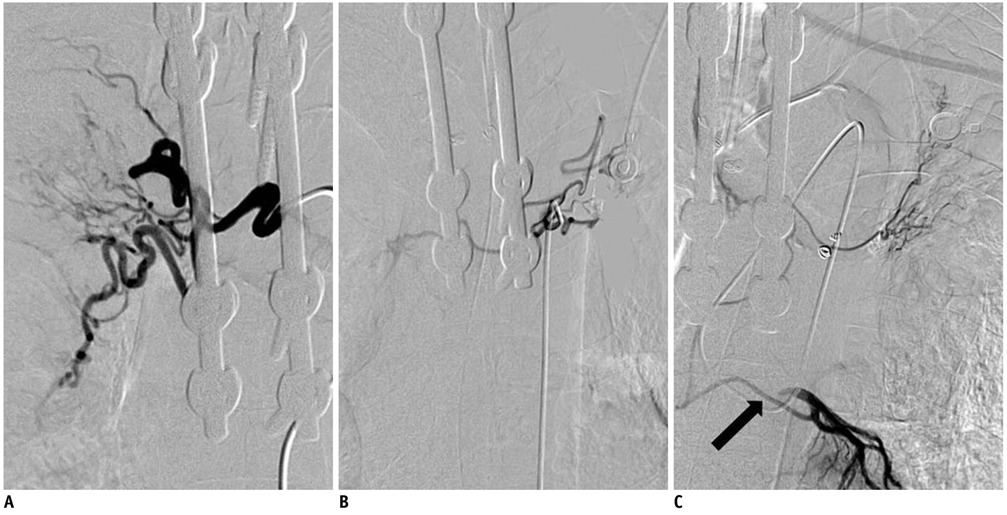
Fig. 1 Angiographies of both bronchial arteries and coronary-to-bronchial artery fistula in 70-year-old male, case 1. A, B. Both bronchial arteries are enlarged and embolized on initial embolization treatments. C. Coronary to bronchial artery fistula (arrow, proximal left circumflex arterial branch) to left upper lung with severe pulmonary artery shunt (not shown) is noted on left coronary angiography.
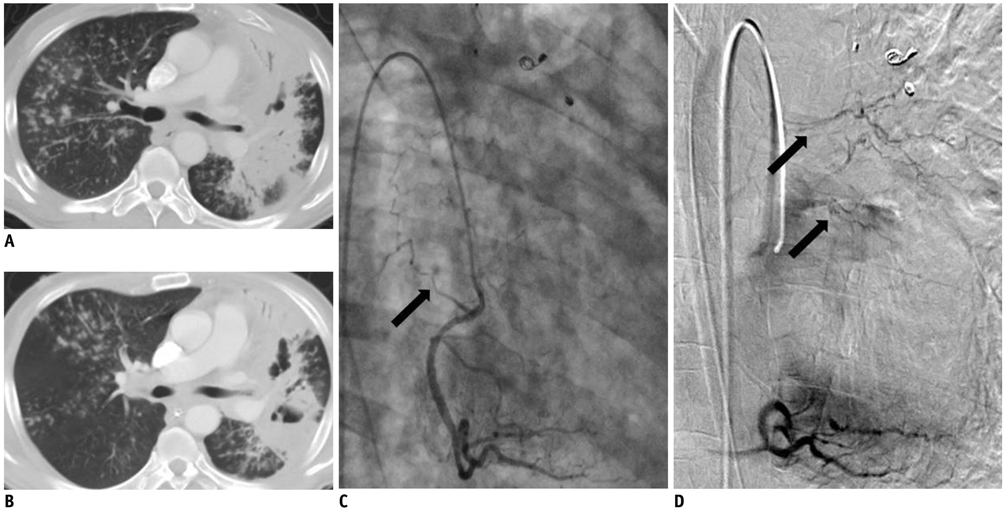
Fig. 2 Chest CT and angiography of right coronary artery in 57-year-old male, case 2. Chest CT images prior to first (A) and second (B) embolization treatments. Right lung lesions were improving but left lung lesions changed into cavitary lesions. Right coronary angiography (C, D) shows coronary to bronchial artery fistula with spastic change from proximal right coronary artery running along superior and inferior walls of left main bronchus (arrows).
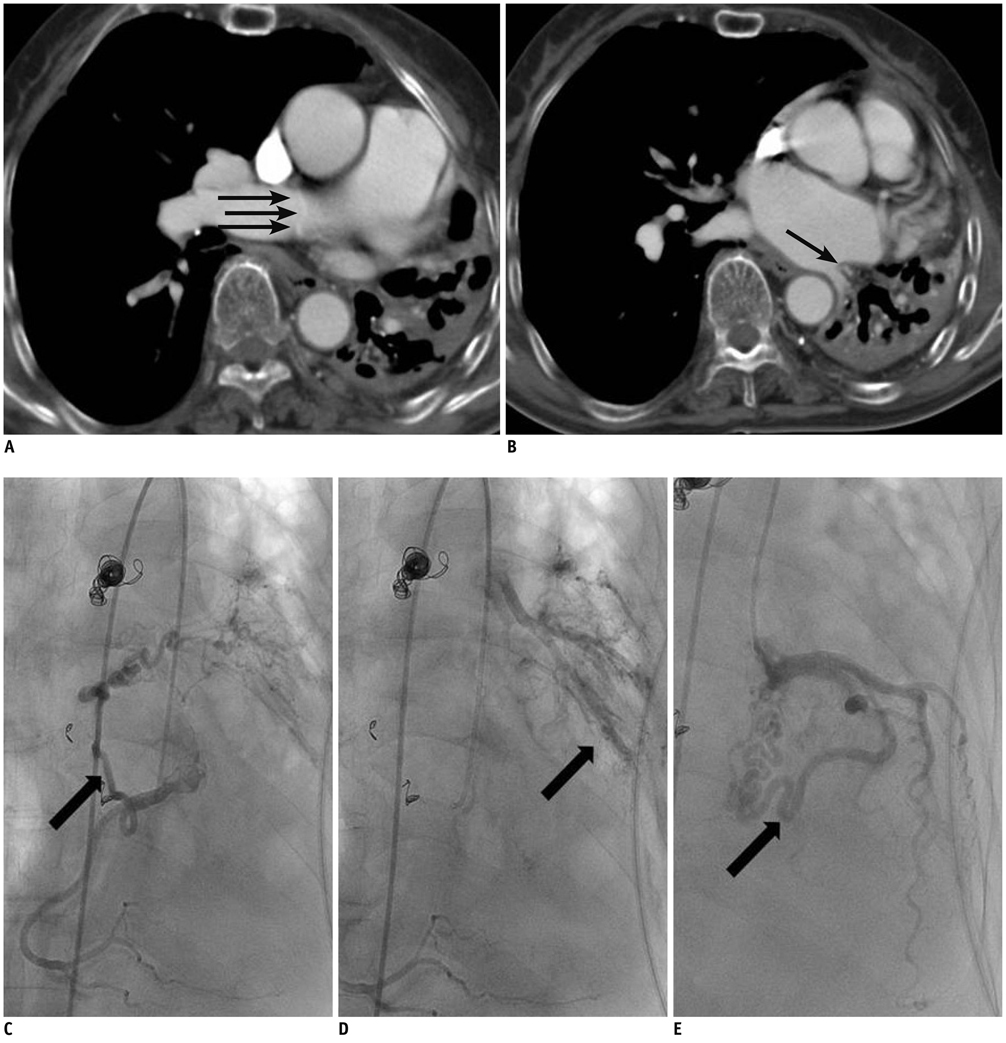
Fig. 3 Chest CT and angiographies of both coronary arteries in 68-year-old female, case 3. A, B. Chest CT images prior to embolization treatment. Small tortuous coronary to bronchial artery fistula is suspected to be traversing right main pulmonary artery (thin arrows, A), and enlarged left and circumflex coronary arteries are seen (thin arrow, B). C, D. Early and late phases of right coronary angiography show enlarged coronary to bronchial artery fistula from proximal right coronary artery and massive pulmonary artery shunt (thick arrows). E. Left coronary angiography shows another enlarged coronary to bronchial artery fistula (thick arrow) that showed severe pulmonary artery shunt at left lower lung (not shown).
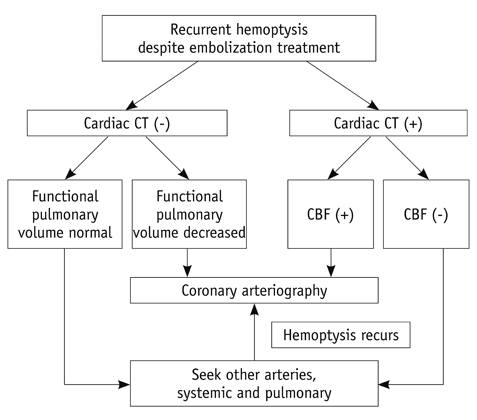
Fig. 4 Diagrammatic representation of work-up and treatment of coronary to bronchial artery fistula. CBF = coronary to bronchial artery fistula
Reference
-
1. Von Haller A. First lines of physiology. 1803. 1st ed. Troy, OH: Penniman;35.2. Lee ST, Kim SY, Hur G, Hwang YJ, Kim YH, Seo JW, et al. Coronary-to-bronchial artery fistula: demonstration by 64-multidetector computed tomography with retrospective electrocardiogram-gated reconstructions. J Comput Assist Tomogr. 2008. 32:444–447.3. Matsunaga N, Hayashi K, Sakamoto I, Ogawa Y, Matsuoka Y, Imamura T, et al. Coronary-to-pulmonary artery shunts via the bronchial artery: analysis of cineangiographic studies. Radiology. 1993. 186:877–882.4. Jim MH, Lee SW, Lam L. Localized bronchiectasis is a definite association of coronaro-bronchial artery fistula. J Invasive Cardiol. 2003. 15:554–556.5. Cho J, Shin T, Jun K, Ryoo J, Choi H, Choi B, et al. Transcatheter embolization of bronchial artery arising from left circumflex coronary artery in a patient with massive hemoptysis. Cardiovasc Intervent Radiol. 2010. 33:169–172.6. Miyazono N, Inoue H, Hori A, Kanetsuki I, Shimada J, Nakajo M. Visualization of left bronchial-to-coronary artery communication after distal bronchial artery embolization for bronchiectasis. Cardiovasc Intervent Radiol. 1994. 17:36–37.7. Peynircioglu B, Ergun O, Hazirolan T, Cil BE, Aytemir K. Bronchial to coronary artery fistulas: an important sign of silent coronary artery disease and potential complication during bronchial artery embolization. Acta Radiol. 2007. 48:171–172.8. Yoon W, Kim JK, Kim YH, Chung TW, Kang HK. Bronchial and nonbronchial systemic artery embolization for life-threatening hemoptysis: a comprehensive review. Radiographics. 2002. 22:1395–1409.9. Jarry G, Bruaire JP, Commeau P, Hermida JS, Leborgne L, Auquier MA, et al. Coronary-to-bronchial artery communication: report of two patients successfully treated by embolization. Cardiovasc Intervent Radiol. 1999. 22:251–254.10. Shin S, Shin TB, Choi H, Choi JS, Kim YH, Kim CW, et al. Peripheral pulmonary arterial pseudoaneurysms: therapeutic implications of endovascular treatment and angiographic classifications. Radiology. 2010. 256:656–664.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pulmonary Artery-bronchial Fistula with Massive Hemoptysis due to Pulmonary Tuberculosis
- Coronary-Bronchial Artery Fistula Manifested by Hemoptysis and Myocardial Ischemia in a Patient with Bronchiectasis
- Bronchial artery embolization: clinical analysis of 129 cases
- Roentgenogram of the Issue ; Massive Hemoptysis in Longstanding Pulmonary Tuberculosis
- Left Circumflex Coronary Artery Fistula Connected to the Right Bronchial Artery Associated with Bronchiectasis: Multidetector CT and Coronary Angiography Findings
