Two Cases of Endobronchial Actinomycosis that were Cured by Operation and Short Term Antibiotics Therapy
- Affiliations
-
- 1Department of Internal Medicine, Soonchunhyang University College of Medicine, Cheonan, Korea. juokna@hanmail.net
- 2Department of Pathology, Soonchunhyang University College of Medicine, Cheonan, Korea.
Abstract
- Endobronchial actinomycosis is a rare chronic suppurative granulomatous infection of the bronchus, and this is sometimes related with a foreign body or a broncholith. The traditional treatment of endobroncial actinomycosis is intravenous antibiotics for 2 to 6 weeks and then oral antibiotics therapy for 6 to 12 months. We report here on 2 cases of endobronchial actinomycosis that were associated with a broncholith and a foreign body, respectively. Surgery followed by short term antibiotics therapy for only 20 days and 34 days, respectively, was effective as treatment for the endobronchial actinomycosis in our cases. After treatment, there were no complications or recurrence during the following period. We suggest that short term antibiotics therapy combined with a surgical operation might be effective as treatment for primary endobronchial actinomycosis, and especially when this illness is combined with a foreign body or a broncholith, as compared with traditional long term antibiotic therapy.
Figure
-
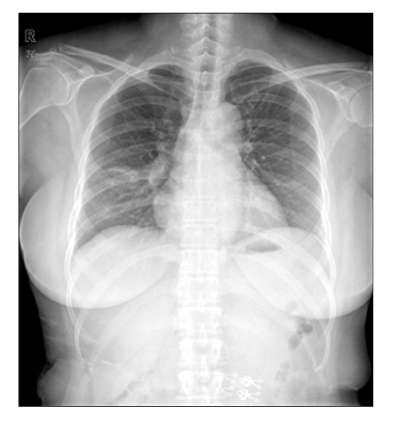
Figure 1 Case 1: Chest radiography showed consolidation at RML (Right middle lobe) lateral segment.

Figure 2 Case 1: Chest computed tomography showed obstructive bronchitis with Bronchiolith in RML (Right middle lobe), lateral segment.
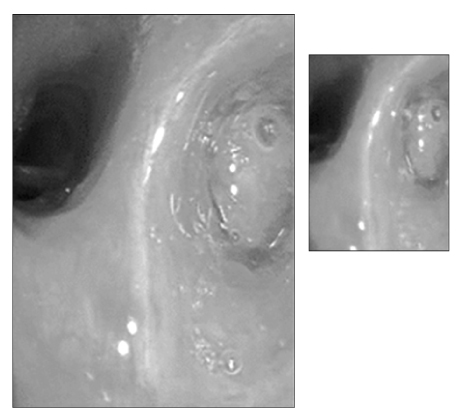
Figure 3 Case 1: Bronchoscopy showed near total obstruction by yellowish hard nodule at RML (Right middle lobe) lateral segment.
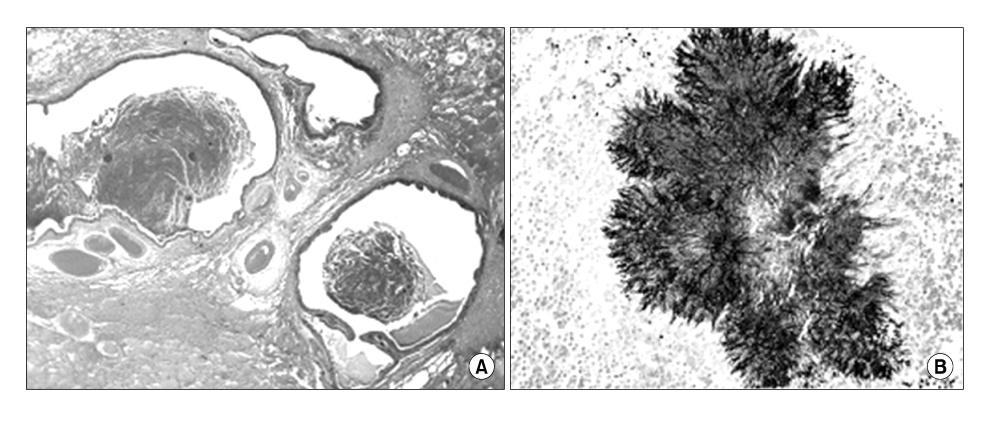
Figure 4 Case 1: Microscopically, (A) the resected lung shows diffuse dilated bronchi or bronchioles containing necrotic material (H&E stain, ×10). (B) An actinomycetes colony composed by radially arranged filamentous bacilli is noted (GMS stain, ×200).
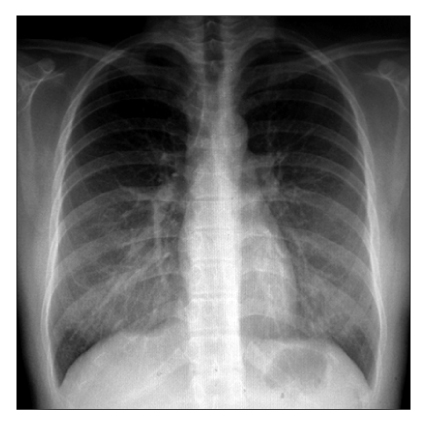
Figure 5 Case 2: Chest radiography showed RML (Right middle lobe) collapse.

Figure 6 Case 2: Bronchoscopy showed near total obstruction of right intermedius branch with a bone like material.
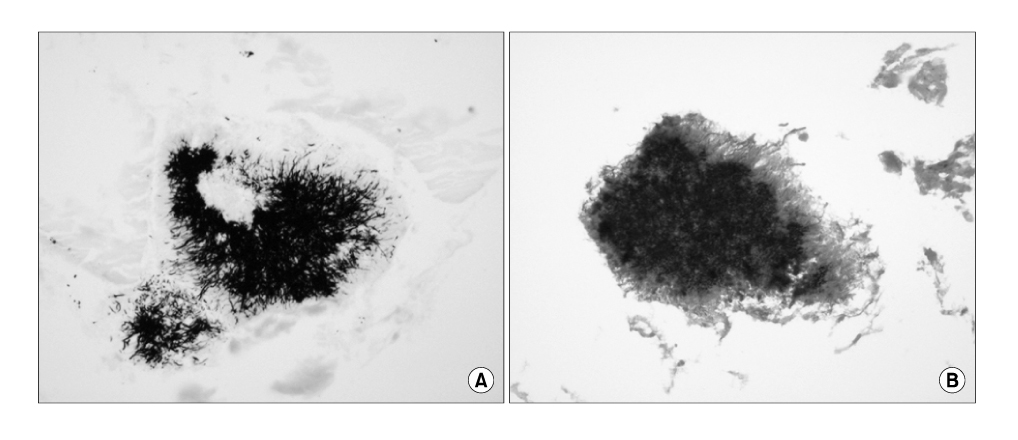
Figure 7 Case 2: Microscopic finding shows actinomycetes colonies, composed by radially arranged filamentous bacilli in (A) (GMS stain, ×100) & (B) (Gram stain, ×100).
Reference
-
1. Brown JR. Human actinomycosis: a study of 181 subjects. Hum Pathol. 1973. 4:319–330.2. Hsieh MJ, Liu HP, Chang JP, Chang CH. Thoracic actinomycosis. Chest. 1993. 149:366–370.3. Russo TA. Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, editors. 156. Actinomycosis. Harrison's principles of internal medicine. 2008. 17th ed. New York: McGraw hill;996–999.4. Dalhoff K, Wallner S, Finck C, Gatermann S, Wiessmann KJ. Endobronchial actinomycosis. Eur Respir J. 1994. 7:1189–1191.5. Choi JC, Koh WJ, Kwon YS, Ryu YJ, Yu CM, Jeon KM, et al. Diagnosis and treatment of endobroncial actinomycosis. Tuberc Respir Dis. 2005. 58:576–581.6. Park JO, Ryu JW, Park S, Kim SH, Seo PW. Broncholithiasis caused by actinomycosis. Korean J Thorac Cardiovasc Surg. 2006. 39:236–239.7. Slade PR, Slesser BV, Southgate J. Thoracic actinomycosis. Thorax. 1973. 28:73–85.8. Goetz MB, Finegold SM. Murray FJ, Nadel JA, editors. Actinomycosis. Textbook of respiratory medicine. 2000. 3rd ed. Philadelphia: W.B.Saunders;1020–1022.9. Dicpinigaitis PV, Bleiweiss IJ, Krellenstein DJ, Halton KP, Teirstein AS. Primary endobronchial actinomycosis in association with foreign body aspiration. Chest. 1992. 101:283–285.10. Ho JC, Ooi GC, Lam WK, Lam B, Cheung TF, Tsang KW. Endobronchial actinomycosis associated with a foreign body. Respirology. 2000. 5:293–296.11. Harvey JC, Cantrell JR, Fisher AM. Actinomycosis: its recognition and treatment. Ann Intern Med. 1957. 46:868–885.12. Seo JB, Lee JW, Ha SY, Park JW, Jeong SH, Park GY. Primary endobronchial actinomycosis associated with broncholithiasis. Respiration. 2003. 70:110–113.13. Hong SB, Kim WS, Lee JH, Bang SJ, Shim TS, Lim CM, et al. Clinical study on thoracic actinomycosis. Tuberc Respir Dis. 1998. 45:1058–1066.14. Yu SE, Ju K, Song SH, Kim CH. A case report of primary endobronchial actinomycosis. Korean J Bronchoesophagol. 2002. 8:56–60.15. Skoutelis A, Petrochilos J, Bassaris H. Successful treatment of thoracic actinomycosis with ceftriaxone. Clin Infect Dis. 1994. 19:161–162.16. Jara FM, Toledo-Pereyra LH, Magilligan DJ Jr. Surgical implications of pulmonary actinomycosis. J Thorac Cardiovasc Surg. 1979. 78:600–604.17. Park K, Kwon JB, Lee JH. Thoracic actinomycosis. Korean J Thorac Cardiovasc Surg. 2005. 38:50–55.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two cases of endobronchial actinomycosis that were cured by bronchoscopic removal and short-term antibiotic therapy
- A Case of Endobronchial Actinomycosis with a Broncholith cured by Cryotherapy through a Flexible Bronchoscope
- Endobronchial actinomycosis simulating endobronchial tuberculosis: a case report
- A clinical study of the treatment of pelvic actinomycosis
- Diagnosis and Treatment of Endobronchial Actinomycosis
