Korean J Urol.
2011 Apr;52(4):269-273.
Comparison of Effectiveness of Monopolar and Bipolar Transurethral Resection of the Prostate and Open Prostatectomy in Large Benign Prostatic Hyperplasia
- Affiliations
-
- 1Department of Urology, Hanyang University College of Medicine, Seoul, Korea. moonuro@hanyang.ac.kr
- 2Department of Urology, Chojung Geriatric Hospital, Cheongwon, Korea.
Abstract
- PURPOSE
Transurethral resection of the prostate (TURP) is still considered the gold standard in the treatment of benign prostatic hyperplasia (BPH). However, open prostatectomy is indicated for prostate glands over 75 ml. There have been few reports concerning the use of TURP for large prostate glands over 100 ml. Herein we compared the effectiveness of monopolar TURP, bipolar TURP, and open prostatectomy in prostate glands larger than 100 ml.
MATERIALS AND METHODS
We reviewed the data of 48 patients with prostate glands larger than 100 ml. A total of 19, 17, and 12 patients underwent monopolar TURP (group A), bipolar TURP (group B), or open prostatectomy (group C), respectively. Preoperative International Prostate Symptom Score (IPSS), maximal flow rate (Qmax), prostate volume, resected tissue volume, resection velocity, and operative time were documented. Postoperative hemoglobin, serum sodium change, hospital stay, and postoperative 6-month IPSS and Qmax were evaluated.
RESULTS
The prostate volumes did not differ significantly among the three groups. Operative time was similar in the two TURP groups, but open prostatectomy required a longer operative time. There was no significant difference in the resected prostate tissue or resection velocity between the two TURP groups. There was a marked decrease in postoperative serum sodium in the monopolar group compared with the other two groups. Among the groups, bipolar TURP required a shorter hospitalization. Postoperative IPSS, quality of life (QoL), and Qmax improved significantly in all groups.
CONCLUSIONS
Even for large prostate glands, the results of this study suggest that bipolar TURP is an effective and safe operation owing to the significant improvements in voiding symptoms, shorter hospitalization, and fewer complications such as transurethral resection syndrome.
MeSH Terms
Figure
-
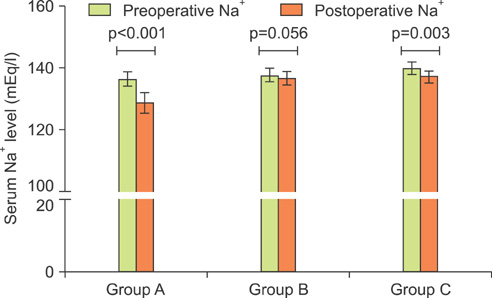
FIG. 1 Perioperative change in serum sodium level among the groups.
Reference
-
1. Lowe FC, McDaniel RL, Chmiel JJ, Hillman AL. Economic modeling to assess the costs of treatment with finasteride, terazosin, and transurethral resection of the prostate for men with moderate to severe symptoms of benign prostatic hyperplasia. Urology. 1995. 46:477–483.2. Barba M, Leyh H, Hartung R. New technologies in transurethral resection of the prostate. Curr Opin Urol. 2000. 10:9–14.3. Tubaro A, Carter S, Hind A, Vicentini C, Miano L. A prospective study of the safety and efficacy of suprapubic transvesical prostatectomy in patients with benign prostatic hyperplasia. J Urol. 2001. 166:172–176.4. Oesterling J. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Retropubic and suprapubic open prostatectomy. Campbell-Walsh urology. 2007. 9th ed. Philadelphia: Saunders;2852.5. Park SW, Chung MK. The results of retropubic prostatectomy and transurethral resection of prostate; compare both results, and then investigate the cause of different results. Korean J Urol. 2004. 45:309–314.6. Kim DK, Kim SJ, Moon HS, Park SY, Kim YT, Choi HY, et al. The role of TURP in the detection of prostate cancer in BPH patients with previously negative prostate biopsy. Korean J Urol. 2010. 51:313–317.7. Holtgrewe HL. Transurethral prostatectomy. Urol Clin North Am. 1995. 22:357–368.8. Mebust WK. Transurethral prostatectomy. Urol Clin North Am. 1990. 17:575–585.9. Mebust WK, Holtgrewe HL, Cockett AT, Peters PC. Transurethral prostatectomy: immediate and postoperative complications. A cooperative study of 13 participating institutions evaluating 3,885 patients. J Urol. 1989. 141:243–247.10. Starkman JS, Santucci RA. Comparison of bipolar transurethral resection of the prostate with standard transurethral prostatectomy: shorter stay, earlier catheter removal and fewer complications. BJU Int. 2005. 95:69–71.11. Eaton AC, Francis RN. The provision of transurethral prostatectomy on a day-case basis using bipolar plasma kinetic technology. BJU Int. 2002. 89:534–537.12. de Sio M, Autorino R, Quarto G, Damiano R, Perdonà S, di Lorenzo G, et al. Gyrus bipolar versus standard monopolar transurethral resection of the prostate: a randomized prospective trial. Urology. 2006. 67:69–72.13. Patel A, Adshead JM. First clinical experience with new transurethral bipolar prostate electrosurgery resection system: controlled tissue ablation (coblation technology). J Endourol. 2004. 18:959–964.14. Bhansali M, Patankar S, Dobhada S, Khaladkar S. Management of large (>60 g) prostate gland: PlasmaKinetic Superpulse (bipolar) versus conventional (monopolar) transurethral resection of the prostate. J Endourol. 2009. 23:141–145.15. Baek M, Paick SH, Lee BK, Kang MB, Lho YS, Jung SI, et al. The efficacy of bipolar transurethral resection of the prostate in patients with large prostates (>80 g) and analysis of the postoperative results based on the resection ratio. Korean J Urol. 2008. 49:1087–1093.16. Kim HG, Lee BK, Paick SH, Lho YS. Efficacy of bipolar transurethral resection of the prostate: comparison with standard monopolar transurethral resection of the prostate. Korean J Urol. 2006. 47:377–380.17. Kim JY, Moon KH, Yoon CJ, Park TC. Bipolar transurethral resection of the prostate: a comparative study with monopolar transurethral resection. Korean J Urol. 2006. 47:493–497.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Long-Term Results of Transurethral Resection of the Prostate for Large Benign Prostatic Hyperplasia: A Comparative Study with Open Prostatectomy
- Efficacy of Bipolar Transurethral Resection of the Prostate: Comparison with Standard Monopolar Transurethral Resection of the Prostate
- Clinical Observation and Comparison Between the Results of Transurethral Resection and Open Prostatectomy on the Benign Prostatic Hypertrophy
- Clinical Observation on Transurethral Resection of Prostate and Suprapubic Prostatectomy for Benign Prostatic Hypertrophy
- Long-term Follow-up of Bipolar Transurethral Resection of the Prostate Compared with Conventional Monopolar Resectoscope for Patients with Benign Prostatic Hyperplasia
