Simple Anchoring of the Penopubic Skin to the Prepubic Deep Fascia in Surgical Correction of Buried Penis
- Affiliations
-
- 1Department of Urology, Bundang Jeasaeng Hospital, Seongnam, Korea. sjhwany@dmc.or.kr
Abstract
- PURPOSE
The aim of this study was to categorize concealed penis and buried penis by preoperative physical examination including the manual prepubic compression test and to describe a simple surgical technique to correct buried penis that was based on surgical experience and comprehension of the anatomical components.
MATERIALS AND METHODS
From March 2007 to November 2010, 17 patients were diagnosed with buried penis after differentiation of this condition from concealed penis. The described surgical technique consisted of a minimal incision and simple fixation of the penile shaft skin and superficial fascia to the prepubic deep fascia, without degloving the penile skin.
RESULTS
The mean age of the patients was 10.2 years, ranging from 8 years to 15 years. The median follow-up was 19 months (range, 5 to 49 months). The mean penile lengths were 1.8 cm (range, 1.1 to 2.5 cm) preoperatively and 4.5 cm (range, 3.3 to 5.8 cm) postoperatively. The median difference between preoperative and postoperative penile lengths was 2.7 cm (range, 2.1 to 3.9 cm). There were no serious intra- or postoperative complications.
CONCLUSIONS
With the simple anchoring of the penopubic skin to the prepubic deep fascia, we obtained successful subjective and objective outcomes without complications. We suggest that this is a promising surgical method for selected patients with buried penis.
Keyword
MeSH Terms
Figure
-

FIG. 1 Categorization of concealed penis and buried penis by preoperative physical examination including the manual prepubic compression test.
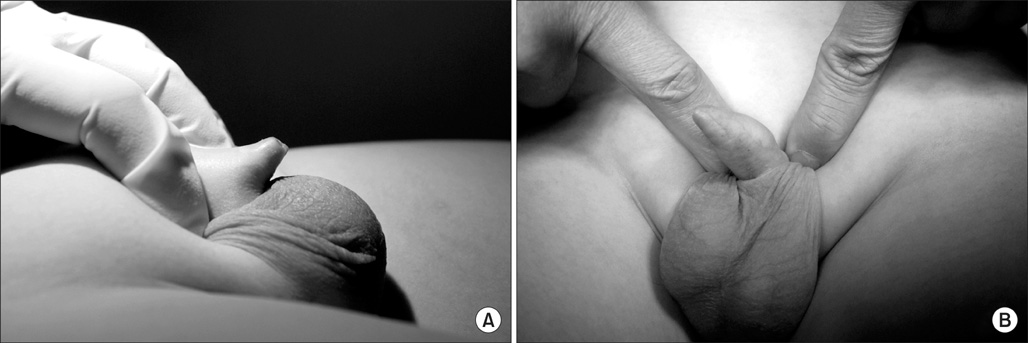
FIG. 2 Comparison between concealed penis (A) and buried penis (B) by use of the manual prepubic compression test.
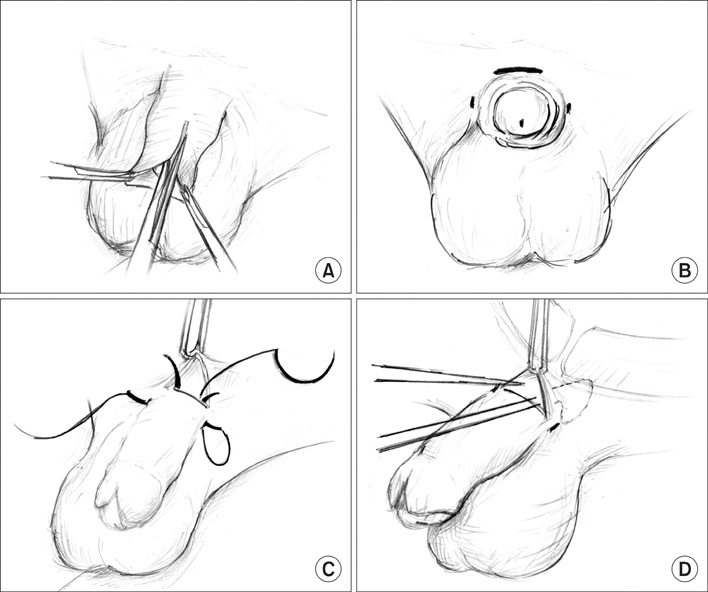
FIG. 3 (A) A dorsal slit incision was made in the midline of the prepuce to expose the whole glans. (B) An approximately 1 cm transverse incision was made near the penile base at 12 o'clock at the penopubic junction. 1 or 2 mm stab incisions at just skin depth were made at the 9 and 3 o'clock positions lateral to the penile shaft. (C) An additional large half-circled needle was tied up to the end of 4-0 nylon and passed through the deep fascia from the 3 o'clock tiny stab incision to the 12 o'clock skin incision. The other end with a 4-0 nylon needle was passed through the subcutaneous tissue from the 3 o'clock tiny stab incision to the 12 o'clock skin incision. (D) After confirming that the penopubic junction was secured to the prepubic deep fascia in the stretched state, each side of the stitch was tied up under the 12 o'clock incision.
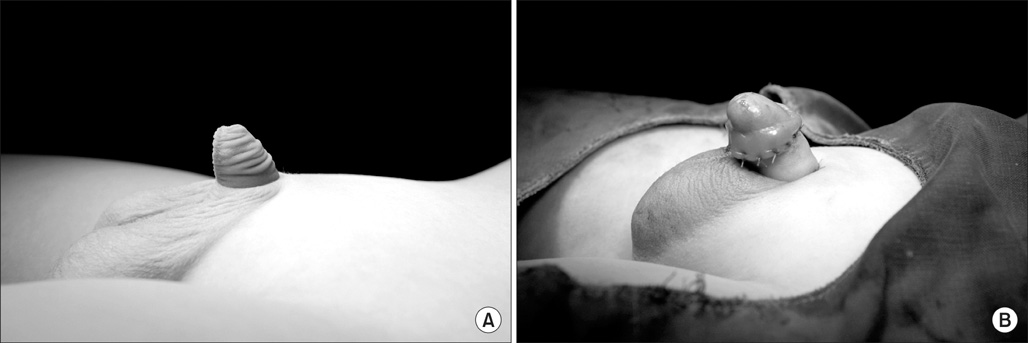
FIG. 4 (A) Preoperative appearance of the buried penis. (B) Immediate postoperative appearance of the buried penis.
Reference
-
1. Lee T, Suh HJ, Han JU. Correcting congenital concealed penis: new pediatric surgical technique. Urology. 2005. 65:789–792.2. Maizels M, Zaontz M, Donovan J, Bushnick PN, Firlit CF. Surgical correction of the buried penis: description of a classification system and a technique to correct the disorder. J Urol. 1986. 136:268–271.3. Alter GJ, Ehrlich RM. A new technique for correction of the hidden penis in children and adults. J Urol. 1999. 161:455–459.4. Yu W, Cheng F, Zhang X, Ruan Y, Yang S, Xia Y. Minimally invasive technique for the concealed penis lead to longer penile length. Pediatr Surg Int. 2010. 26:433–437.5. Redman JF. Buried penis: congenital syndrome of a short penile shaft and a paucity of penile shaft skin. J Urol. 2005. 173:1714–1717.6. Wollin M, Duffy PG, Malone PS, Ransley PG. Buried penis. A novel approach. Br J Urol. 1990. 65:97–100.7. Frenkl TL, Agarwal S, Caldamone AA. Results of a simplified technique for buried penis repair. J Urol. 2004. 171:826–828.8. Elder JS. Wein AJ, Kavoussi LR, Novik AC, Partin AW, Peters CA, editors. Abnormalities of the genitalia in boys and their surgical management. Campbell-Walsh urology. 2007. 9th ed. Philadelphia: Saunders;3745–3760.9. Oh CY, Lee Hy, Hong CH, Han Sw. Long-term outcome and parents satisfaction after the correction of concealed penis. Korean J Pediatric Urol. 2009. 1:58–63.10. Shaeer O, Shaeer K. Revealing the buried penis in adults. J Sex Med. 2009. 6:876–885.11. Wood D, Woodhouse C. Penile anomalies in adolescence. ScientificWorldJournal. 2011. 11:614–623.12. Kim JS, Seo IY. Surgical correction of concealed penis by suprapubic lipectomy and a modification of johnston's principle under local anesthesia. Korean J Urol. 2000. 41:1023–1032.13. Moon SY, Jung GW, Yoon JH. New method of correction for severe or recurrent concealed penis after operation by conventional method. Korean J Urol. 1998. 39:1047–1050.14. Park SW, Lee SD. Long-term parental satisfaction after surgical treatment of concealed penis. Korean J Urol. 2008. 49:627–632.15. Mattsson B, Vollmer C, Schwab C, Padevit C, Horton K, John H, et al. Complications of a buried penis in an extremely obese patient. Andrologia. 2011. Epub ahead of print.16. Brisson P, Patel H, Chan M, Feins N. Penoplasty for buried penis in children: report of 50 cases. J Pediatr Surg. 2001. 36:421–425.17. Borsellino A, Spagnoli A, Vallasciani S, Martini L, Ferro F. Surgical approach to concealed penis: technical refinements and outcome. Urology. 2007. 69:1195–1198.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Concealed Penis: Adjunctive Suprapubic Lipectomy
- Clinical Experience of Concealed Penis
- New Method of Correction for Severe or Recurrent Concealed Penis after Operation by Conventional Method
- Preputial Stones as a Rare Complication of Buried Penis: A Case Report
- Repair of Transected Penis and Perineal Injury Using Gracilis and Tensor Fascia Lata Myocutaneous Flap
