Korean J Urol.
2010 Apr;51(4):276-280.
The Clinical Significance of a Retroaortic Left Renal Vein
- Affiliations
-
- 1Department of Urology, Pusan National University School of Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea. lsd@pusan.ac.kr
Abstract
- PURPOSE
A retroaortic left renal vein (RLRV) is located between the aorta and the vertebra and drains into the inferior vena cava. Urological symptoms can be caused by increased pressure in the renal vein. To evaluate the clinical importance of RLRV, we reviewed patients' medical records and radiologic findings. MATERIALS AND METHODS: Nine patients who were studied with multidetector computed tomography at our institution from January 2003 to December 2009 had urologic symptoms with RLRV. We retrospectively reviewed these patients' medical records and analyzed their clinical characteristics. RESULTS: The patients' mean age was 46.0+/-20.1 years (range, 17-65 years) and the male to female ratio was 5 to 4. The urologic symptoms of the initial diagnosis were various (hematuria: 5 of the 9 patients; left flank pain: 4 of the 9 patients; inguinal pain: 1 of the 5 male patients; and gross hematuria: 1 of the 9 patients). The distribution among the type I, II, III, and IV of RLRV was 6, 2, 1, and 0 patients, respectively. The concomitant diseases were ureteropelvic junction obstruction (UPJO; 2 of the 9 patients) and varicocele (2 of the 5 male patients). One patient with UPJO underwent pyeloplasty and the other patient with UPJO underwent nephrectomy due to a nonfunctional atrophied kidney. The microscopic hematuria was not resolved with conservative management for long-term follow-up. CONCLUSIONS: Hematuria and inguinal or flank pain seem to be common in patients with RLRV. The most common type of RLRV was type I. It appeared that the microscopic hematuria continued in the long-term follow-up.
Keyword
MeSH Terms
Figure
-
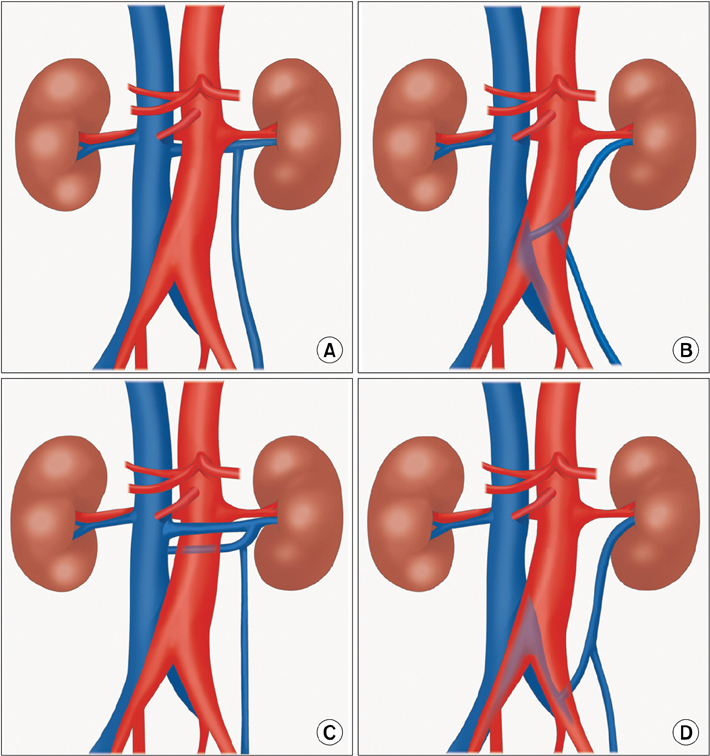
FIG. 1 Schematic illustration of the different types of retroaortic left renal vein anomalies. (A) type I, (B) type II, (C) type III, (D) type IV.
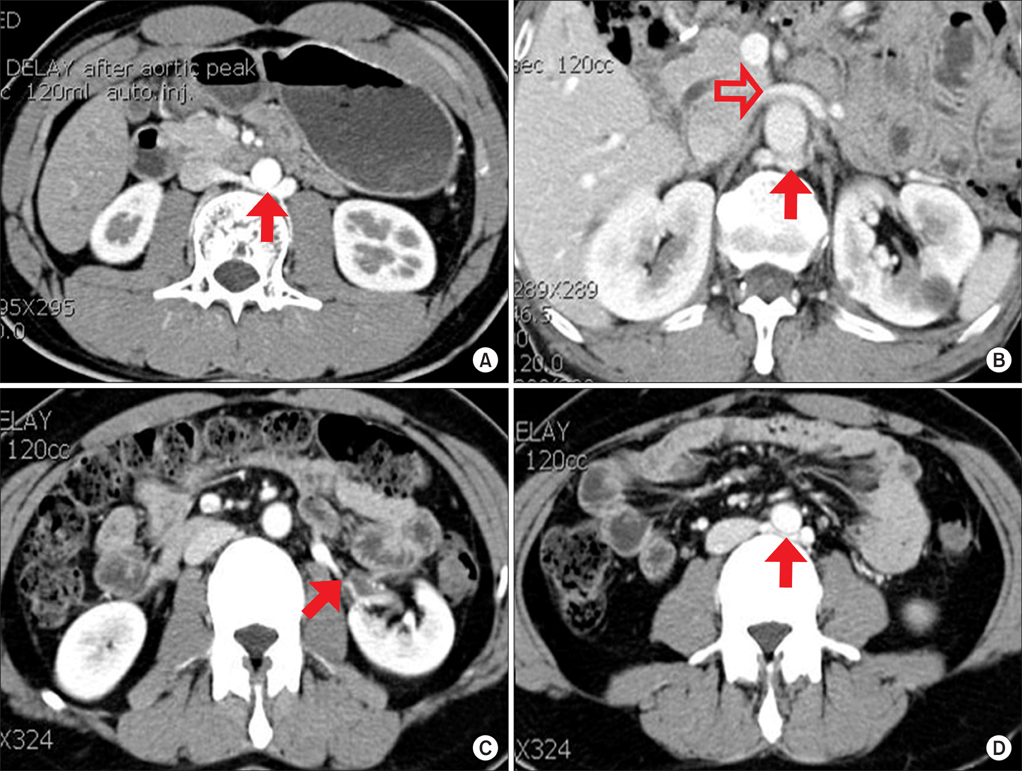
FIG. 2 Type I, II, and III of RLRV. (A) Type I of RLRV (arrow). (B) Type III of RLRV. The superior left renal vein (open arrow) and inferior left renal vein (arrow) crossed anterior and posterior to the aorta. (C, D) Ureteropelvic junction obstruction with type II of RLRV. Anteromedial crossing vessel (arrow in C) and joining IVC (arrow in D) at level L4. RLRV: retroaortic left renal vein, IVC: inferior vena cava.
Reference
-
1. Mayo J, Gray R, St Louis E, Grosman H, McLoughlin M, Wise D. Anomalies of the inferior vena cava. AJR Am J Roentgenol. 1983. 140:339–345.2. Royal SA, Callen PW. CT evaluation of anomalies of the inferior vena cava and left renal vein. AJR Am J Roentgenol. 1979. 132:759–763.3. Hayashi M, Kume T, Nihira H. Abnormalities of renal venous system and unexplained renal hematuria. J Urol. 1980. 124:12–16.4. Thomas TV. Surgical implications of retroaortic left renal vein. Arch Surg. 1970. 100:738–740.5. Cuéllar i Calàbria H, Quiroga Gómez S, Sebastia Cerquedà C, Boyé de la Presa R, Miranda A, Alvarez-Castells A. Nutcracker or left renal vein compression phenomenon: multidetector computed tomography findings and clinical significance. Eur Radiol. 2005. 15:1745–1751.6. Karaman B, Koplay M, Ozturk E, Basekim CC, Ogul H, Mutlu H, et al. Retroaortic left renal vein: multidetector computed tomography angiography findings and its clinical importance. Acta Radiol. 2007. 48:355–360.7. Shindo S, Kubota K, Kojima A, Iyori K, Ishimoto T, Kobayashi M, et al. Anomalies of inferior vena cava and left renal vein: risks in aortic surgery. Ann Vasc Surg. 2000. 14:393–396.8. Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH Jr. Spectrum of congenital anomalies of the inferior vena cava: cross-sectional imaging findings. Radiographics. 2000. 20:639–652.9. Mathews R, Smith PA, Fishman EK, Marshall FF. Anomalies of the inferior vena cava and renal veins: embryologic and surgical considerations. Urology. 1999. 53:873–880.10. Karkos CD, Bruce IA, Thomson GJ, Lambert ME. Retroaortic left renal vein and its implications in abdominal aortic surgery. Ann Vasc Surg. 2001. 15:703–708.11. Minniti S, Visentini S, Procacci C. Congenital anomalies of the venae cavae: embryological origin, imaging features and report of three new variants. Eur Radiol. 2002. 12:2040–2055.12. Hoeltl W, Hruby W, Aharinejad S. Renal vein anatomy and its implications for retroperitoneal surgery. J Urol. 1990. 143:1108–1114.13. Kraus GJ, Goerzer HG. MR-angiographic diagnosis of an aberrant retroaortic left renal vein and review of the literature. Clin Imaging. 2003. 27:132–134.14. Trigaux JP, Vandroogenbroek S, De Wispelaere JF, Lacrosse M, Jamart J. Congenital anomalies of the inferior vena cava and left renal vein: evaluation with spiral CT. J Vasc Interv Radiol. 1998. 9:339–345.15. Lee SE, Park DS, Chung SY, Lee YT. Retroaortic renal vein. Korean J Urol. 2002. 43:84–86.16. Gibo M, Onitsuka H. Retroaortic left renal vein with renal vein hypertension causing hematuria. Clin Imaging. 1998. 22:422–424.17. Hohenfellner M, Steinbach F, Schultz-Lampel D, Schantzen W, Walter K, Cramer BM, et al. The nutcracker syndrome: new aspects of pathophysiology, diagnosis and treatment. J Urol. 1991. 146:685–688.18. Rudloff U, Holmes RJ, Prem JT, Faust GR, Moldwin R, Siegel D. Mesoaortic compression of the left renal vein (nutcracker syndrome): case reports and review of the literature. Ann Vasc Surg. 2006. 20:120–129.19. Graif M, Hauser R, Hirshebein A, Botchan A, Kessler A, Yabetz H. Varicocele and the testicular-renal venous route: hemodynamic Doppler sonographic investigation. J Ultrasound Med. 2000. 19:627–631.20. Takahashi Y, Ohta S, Sano A, Kuroda Y, Kaji Y, Matsuki M, et al. Does severe nutcracker phenomenon cause pediatric chronic fatigue? Clin Nephrol. 2000. 53:174–181.21. Scultetus AH, Villavicencio JL, Gillespie DL. The nutcracker syndrome: its role in the pelvic venous disorders. J Vasc Surg. 2001. 34:812–819.22. Van Cangh PJ, Wilmart JF, Opsomer RJ, Abi-Aad A, Wese FX, Lorge F. Long-term results and late recurrence after endoureteropyelotomy: a critical analysis of prognostic factors. J Urol. 1994. 151:934–937.23. Nakada SY, Wolf JS Jr, Brink JA, Quillen SP, Nadler RB, Gaines MV, et al. Retrospective analysis of the effect of crossing vessels on successful retrograde endopyelotomy outcomes using spiral computerized tomography angiography. J Urol. 1998. 159:62–65.24. Keeley FX Jr, Moussa SA, Miller J, Tolley DA. A prospective study of endoluminal ultrasound versus computerized tomography angiography for detecting crossing vessels at the ureteropelvic junction. J Urol. 1999. 162:1938–1941.25. Braun P, Guilabert JP, Kazmi F. Multidetector computed tomography arteriography in the preoperative assessment of patients with ureteropelvic junction obstruction. Eur J Radiol. 2007. 61:170–175.26. Cho BC, Choi HJ, Kang SM, Chang J, Lee SM, Yang DG, et al. Congenital absence of inferior vena cava as a rare cause of pulmonary thromboembolism. Yonsei Med J. 2004. 45:947–951.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multi-Detector CT Findings of Double Retroaortic Left Renal Veins
- Retroaortic Renal Vein
- Posterior Nutcracker Syndrome Associated with Interrupted Left Inferior Vena Cava with Azygos Continuation and Retroaortic Right Renal Vein
- Retroaortic Course and Azygous Continuation of an Aberrant Left Brachiocephalic Vein
- The Incidence of Inferior Vena Cava Anomalies by MDCT
