Renal Ruptures with Active Bleeding Treated with Emergency Selective Renal Arterial Embolization
- Affiliations
-
- 1Department of Urology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. rjpark@uuh.ulsan.kr
- 2Department of Radiology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
Abstract
- Selection of a treatment modality for traumatized renal rupture depends on the renal injury grade, hemodynamic stability, combined organ injury, and the physician's experience. Treatment for renal injury tends to be conservative to maintain renal function and lessen the morbidity of surgery. If renal injuries were well-staged and selected by radiologic evaluation, hemodynamically stable patients with significant injuries (grades II through V) can usually be managed without surgical exploration. We report 3 cases of grade 4 renal injuries successfully treated with selective renal arterial embolization.
Keyword
Figure
-
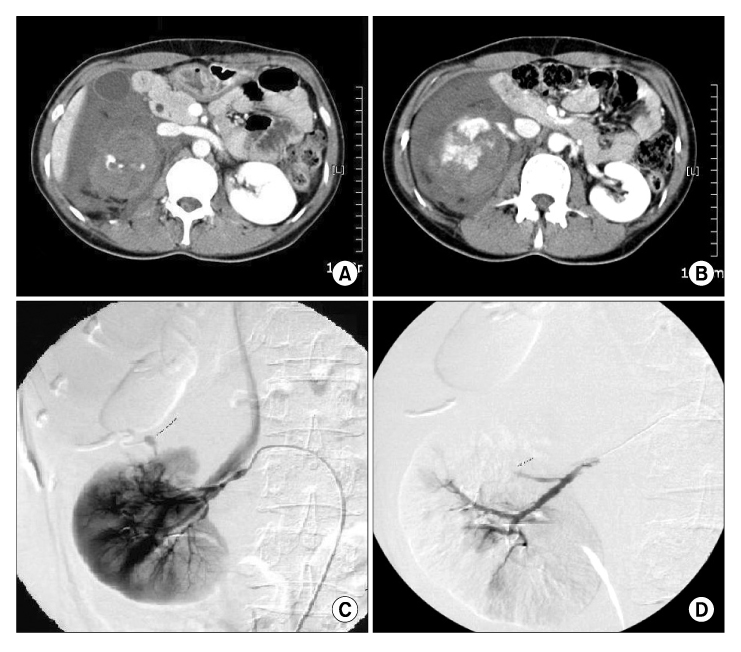
Fig. 1 A 34-year-old woman. (A) and (B) show active bleeding at the injured kidney, suggesting grade IV renal injury on CT scan. (C) shows pseudoaneurysm and blood extravasation suggesting, active bleeding of the kidney on angiography. (D) shows the picture that there was no extravasation after selective embolization.

Fig. 2 A 41-year-old man. (A) and (B) show active bleeding at the injured kidney, suggesting grade IV renal injury on CT scan. (C) shows pseudoaneurysm and blood extravasation suggesting, active bleeding of the kidney on angiography. (D) shows the picture that there was no extravasation after selective embolization.

Fig. 3 A 16-year-old boy. (A) and (B) show active bleeding at the injured kidney, suggesting grade IV renal injury on CT scan. (C) shows pseudoaneurysm and blood extravasation, suggesting active bleeding of the kidney on angiography. (D) shows that there was no extravasation after selective embolization.
Reference
-
1. Sofocleous CT, Hinrichs C, Hubbi B, Brountzos E, Kaul S, Kannarkat G, et al. Angiographic findings and embolotherapy in renal arterial trauma. Cardiovasc Intervent Radiol. 2005. 28:39–47.2. McAninch JW, Resnick MI. Genitourinary trauma. Urol Clin North Am. 2006. 33:13–19.3. McAninch JW, Santucci RA. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Renal and ureteral trauma. Campbell-Walsh urology. 2007. 9th ed. Philadelphia: Saunders;1274–1292. .4. Kim HS, Ryu SB, Min BK. A case of control of renal hemorrhage by selective renal arterial embolization. Korean J Urol. 1988. 29:324–328.5. Moudouni SM, Patard JJ, Manunta A, Guiraud P, Guille F, Lobel B. A conservative approach to major blunt renal lacerations with urinary extravasation and devitalized renal segments. BJU Int. 2001. 87:290–294.6. Kim DH, Jeon YS, Lee NK. Grade IV and V renal injury: how to treat? Korean J Urol. 2002. 43:727–732.7. Chuang VP, Wallace S, Swanson DA. Technique and complications of renal carcinoma infarction. Urol Radiol. 1981. 2:223–228.8. Fischer RG, Ben-Menachem Y, Whigham C. Stab wounds of the renal artery branches: angiographic diagnosis and treatment by embolization. AJR Am J Roentgenol. 1989. 152:1231–1235.9. Altman AL, Haas C, Dinchman KH, Spirnak JP. Selective nonoperative management of blunt grade 5 renal injury. J Urol. 2000. 164:27–30.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Control of Renal Hemorrhage by Selective Renal Arterial Embolization
- Transcatheter arterial embolization for congenital renal arteriovenous fistula
- A Case of Congenital Renal Arteriovenous Fistula
- Selective Arterial Embolization of Renal Arteriovenous Fistula and Arterial Aneurysm
- Renal Arterial Embolization in Metastatic Renal Cell Carcinoma with Absolute Ethanol
