A Patient with Hinman's Syndrome who Underwent Renal Transplantation Using a Pre-existing Cutaneous Ureterostomy
- Affiliations
-
- 1Department of Urology, College of Medicine, Daegu Catholic University, Daegu, Korea jspark@cu.ac.kr
- 2Department of General Surgery, College of Medicine, Daegu Catholic University, Daegu, Korea.
- 3Department of Internal Medicine, College of Medicine, Daegu Catholic University, Daegu, Korea.
Abstract
- It is known that many renal transplantation candidates with end stage renal disease have bladder dysfunction. Before 1966, these patients were considered poor candidates for renal transplantation because of their many bladder problems. But it has recently been reported that renal transplantation with an ileal conduit could solve these problems. Herein, we report on a patient with Hinman's syndrome and this patient underwent renal transplantation using a pre-existing cutaneous ureterostomy.
MeSH Terms
Figure
-
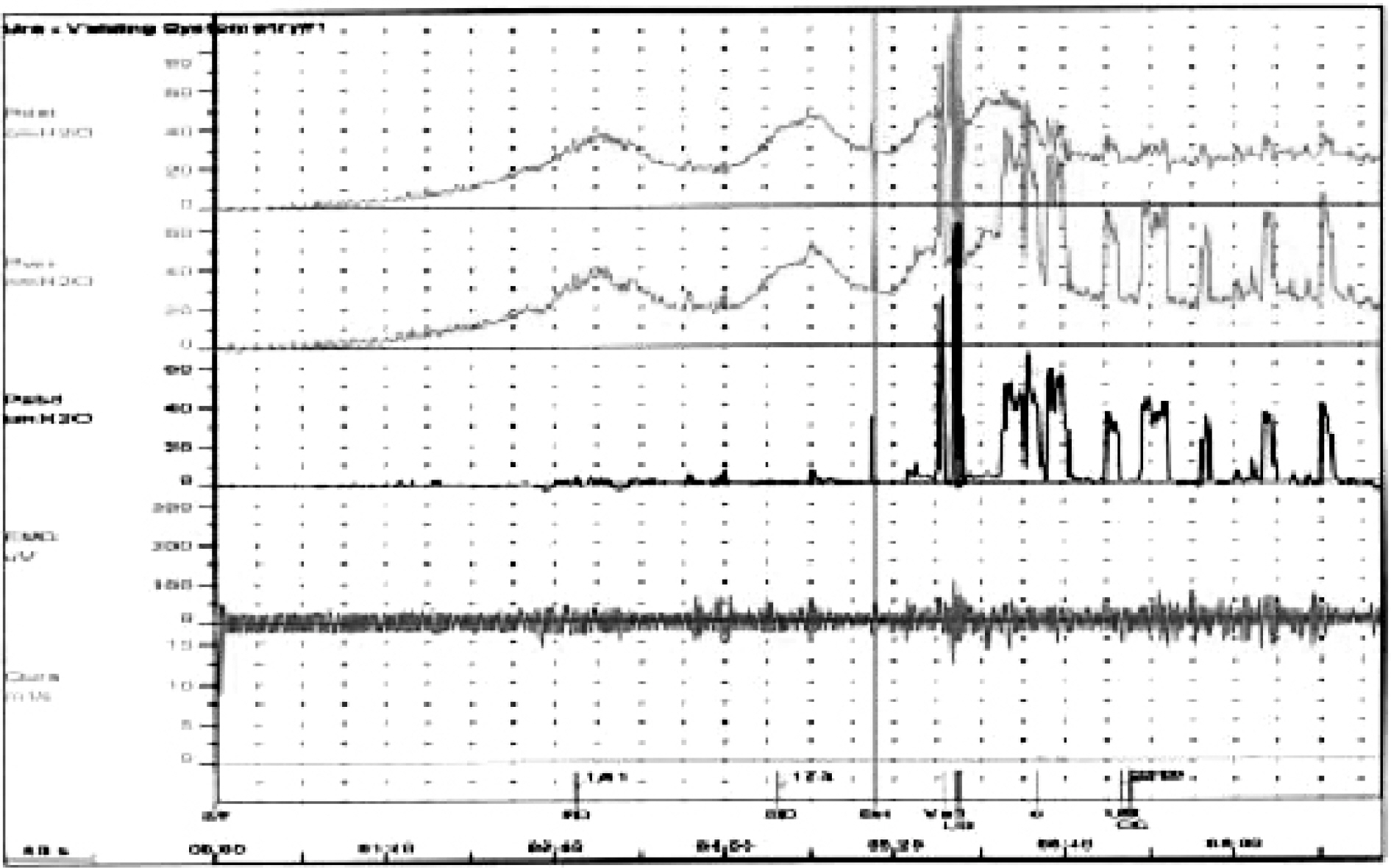
Fig. 1. Urodynamic study (UDS) shows staccato voiding with detrusor hypereflexia and detrusor-sphincter dyssynergia.

Fig. 2. The pre-kidney transplantation (Pre-KT) cystogram shows a 180cc bladder capacity and an improved bladder shape compared with the previous voiding cystourethrogram (VCUG).

Fig. 3. Cutaneous retrograde ureterography. (A) Before transplantation: Cutaneous ureterostomy with transureteroureterostomy in the right lower abdomen. (B) After transplantation: the transplanted ureter was connected to the native left ureter, which drains well into the cutaneous ureterostomy.
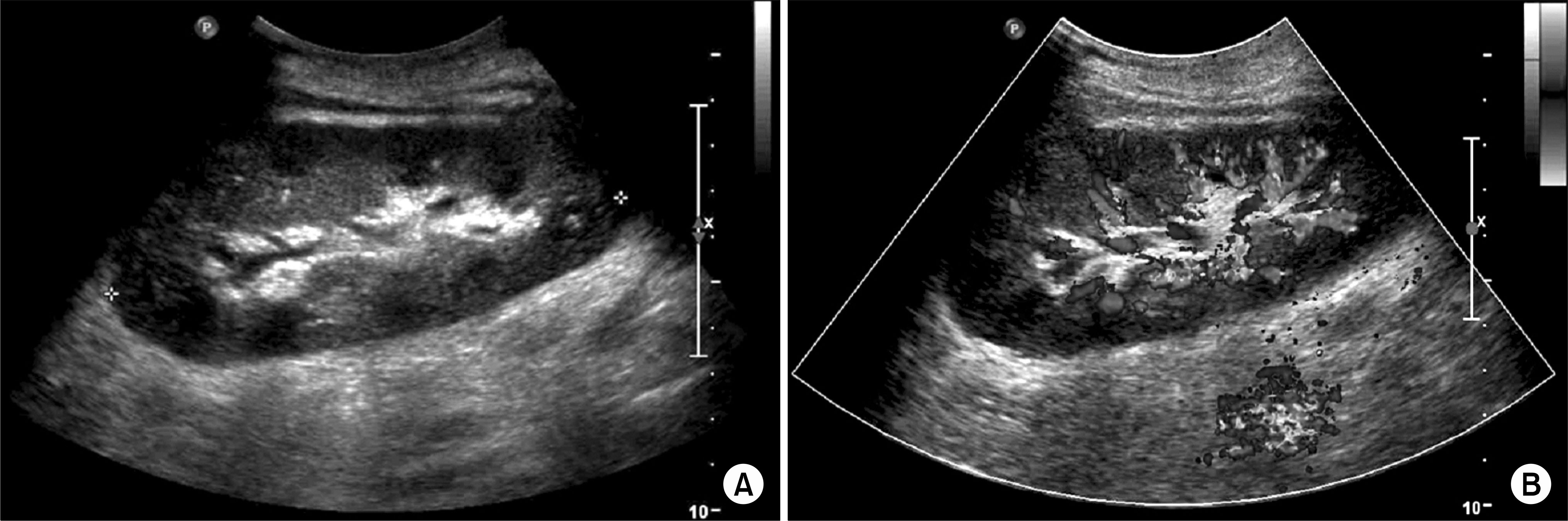
Fig. 4. (A) Kidney ultrasonography: 9 weeks after kidney transplantation (KT), the graft kidney shows normal findings without hydronephrosis. (B) Color doppler kidney ultrasonography (USG): the graft kidney show normal blood flow.
Reference
-
1. Hinman F, Baumann FW. Vesical and ureteral damage from voiding dysfunction in boys with neurologic or obstructive disease. J Urol. 1973; 109:727–32.2. Kelly WD, Merkel FK, Markland C. Ileal urinary diversion in conjunction with renal homotransplantation. Lancet. 1966; 1:222–6.
Article3. Levitt SB, Caberwal D, Kogan SJ, Romas NA, Hardy MA. Use of pre-existing ureterocutaneous anastomosis as conduit in renal allotransplantation. Urology. 1979; 13:377–82.
Article4. Kim SJ, Bang HY, Kim ST, Lee SE. Renal transplantation using ileal conduit. J Korean Soc Transplant. 1991; 5:113–6.5. Williams JL, Confer DJ, DeLemos RA, Monite JE. Colon conduit in pediatric renal transplantation. J Urol. 1980; 124:515–8.
Article6. Shick E, Tanagho EA. The effect of gravity on ureteral peristalsis. J Urol. 1973; 109:187–91.7. Glass NR, Uehling D, Sollinger H, Belzer F. Renal transplantation using ileal conduit in 5 cases. J Urol. 1985; 133:666–8.8. Santiago-Delpin EA, Acosta-Otero A, Vazquez-Lugo A. Ureteral implantation in the kidney transplantation: the use of a mature end ureterostomy. J Urol. 1980; 124:513–4.9. Purohit RS, Bretan PN Jr. Successful longterm outcome using existing native cutaneous ureterostomy for renal transplant drainage. J Urol. 2000; 163:446–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluations for Hydronephrosis After the Establishment of Tubeless Cutaneous Ureterostomy
- Diagnostic Criteria for Stomal Obstruction of Tubeless Cutaneous Ureterostomy by Use of 99mTc-Mercaptoacetyltriglycine Diuretic Renography
- Hinman Syndrome: Long Term Follow up of 14 Case
- A clinical experience of urinary diversion: postoperative complications of diversion
- Experiences with Cutaneous Transureteroureterostomy
