Korean J Urol.
2008 Dec;49(12):1158-1160.
Xanthogranulomatous Pyelonephritis with Spontaneous Nephrocutaneous Fistula
- Affiliations
-
- 1Department of Urology, Soonchunhyang University College of Medicine, Seoul, Korea. wonjya@hosp.sch.ac.kr
- 2Department of Pathology, Soonchunhyang University College of Medicine, Seoul, Korea.
Abstract
- Fistula formation between the upper urinary tract and cutaneous tissue is an uncommon complication in urogenital disease. Xanthogranulomatous pyelonephritis(XGP) is a severe, chronic infection of the renal parenchyma that is often associated with calculi and obstruction. We present a rare case of XGP with a nephrocutaneous fistula.
Figure
-
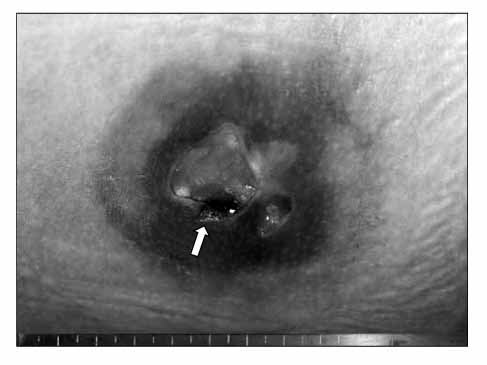
Fig. 1 There is a 4×4cm sized area of necrotic skin change with a fistula opening (arrow) in the right flank area.

Fig. 2 (A) The CT scan shows a fistula tract (arrow) from the lower pole of the right kidney to the right flank area. (B, C) A nephrocutaneous fistula arising from the lower pole of the right kidney (arrow head) and a retroperitoneal abscess (arrow) along the psoas muscle are observed.

Fig. 3 (A) The coronally sectioned kidney shows the fistula opening (arrow) in the lower pole and multiple dilated calyces containing yellowish pus. (B) The microscopic findings show lipid that contains foamy macrophages (arrow) (H&E, ×400).
Reference
-
1. Caberwal D, Katz J, Reid R, Newman HR. A case of nephrobronchial and colonobronchial fistula presenting as lung abscess. J Urol. 1977. 117:371–373.2. Calvo Quintero JE, Alcover Garcia J, Gutierrez Del Pozo R, Pedemonte Vives J, Romero Martin JA, Corominas Estrella S, et al. Fistulization in xanthogranulomatous pyelonephritis. Presentation of 6 clinical cases and review of the literature. Actas Urol Esp. 1989. 13:363–367.3. Rao MS, Bapna BC, Rajendran LJ, Shrikhande VV, Prasanna A, Subudhi CL, et al. Operative management problems in nephrobronchial fistula. Urology. 1981. 17:362–363.4. Kim ME, Kim SJ, Shim BS, Lee GH, Cho YH, Cho IR. Han SW, Kim KS, Kim DY, Kim SJ, Kim JC, Kim HJ, editors. Infection and inflammation. Urology. 2007. 4th ed. Seoul: Ilchokak Publishing Inc;149–216.5. Kim YJ, Huh JS. Clinical characteristics of xanthogranulomatous pyelonephritis. Korean J Urol. 2004. 45:935–940.6. Arango O, Rosales A, Gelabert A. Xanthogranulomatous pyelonephritis with nephrocutaneous fistula at the knee. Br J Urol. 1991. 67:654–655.7. Biyani CS, Torella F, Cornford PA, Brough SJ. Xanthogranulomatous pyelonephritis with bilateral nephrocutaneous fistulae. Urol Int. 1997. 59:46–47.8. Kiris A, Kocakoc E, Poyraz AK, Dagli F, Boztosun Y. Xanthogranulomatous pyelonephritis with nephrocutanous fistula and coexisting renal replacement lipomatosis: the report of a rare case. Clin Imaging. 2005. 29:356–358.9. Srinivasan A, Mowad JJ. Pyelocutaneous fistula after SWL of xanthogranulomatous pyelonephritic kidney: case report. J Endourol. 1998. 12:13–14.10. Choi WJ, Ku JH, Shim HB. Risk factors for urinary stone formation in male patients with spinal cord injury: a 17-year follow-up study. Korean J Urol. 2006. 47:807–812.
