The Use of Cardiac Magnetic Resonance in Patients with Suspected Coronary Artery Disease: A Clinical Practice Perspective
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Heart Vascular Stroke Institute Imaging Center, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 2Duke Cardiovascular Magnetic Resonance Center, Durham, NC, USA. raymond.kim@duke.edu
- 3Department of Medicine, Duke University Medical Center, Durham, NC, USA.
- 4Department of Radiology, Duke University Medical Center, Durham, NC, USA.
- KMID: 2308694
- DOI: http://doi.org/10.4250/jcu.2016.24.2.96
Abstract
- Cardiac magnetic resonance imaging (CMR) is a useful diagnostic imaging modality in patients with known or suspected coronary artery disease (CAD). It provides unique information not available from other modalities, however, it is complex. CMR is not a single technique. Instead, it consists of multiple distinct techniques and a lack of understanding of which techniques to perform and how to interpret the findings in combination limits its efficacy and widespread use. Conversely, its multiparametric nature can provide a comprehensive assessment with the potential for higher accuracy than is achievable by other modalities. Moreover, its ability to directly assess myopathic processes often contributes insights that change patient management. In this article we provide a brief technical overview and focus on specific clinical scenarios in patients with known or suspected CAD. We highlight the multiparametric nature of CMR and discuss cases which illustrate the unique information that CMR can contribute.
MeSH Terms
Figure
-
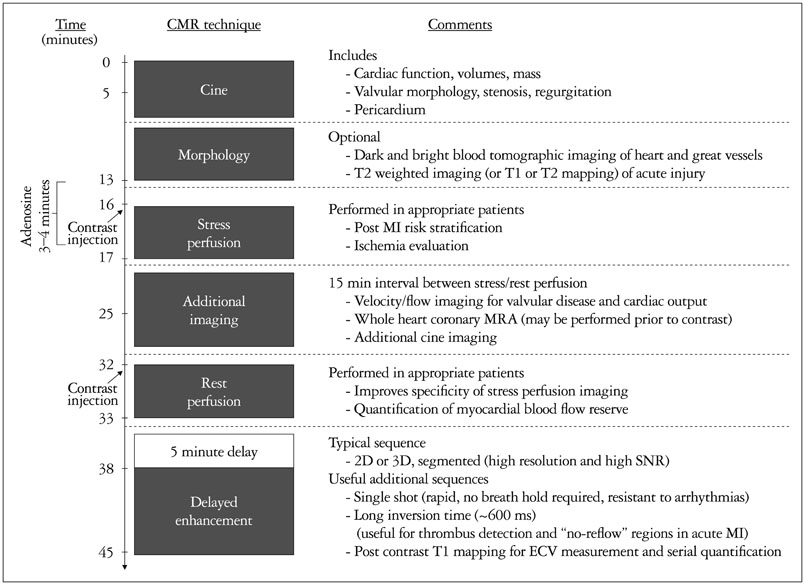
Fig. 1 Timeline and potential components of a multitechnique CMR examination including stress and rest perfusion imaging. Note that the entire exam can be performed within 30–45 minutes. In cases where the patient is unable to cooperate, the cine examination can be performed with real-time imaging and delayed enhancement with single-shot techniques. This technique will reduce artifacts in patients unable to breath-hold and total exam time will be shortened further. Adapted from Kim et al. J Am Coll Cardiol 2009;55:1-16, with permission of Elsevier.1) CMR: cardiac magnetic resonance imaging, MI: myocardial infarction, MRA: magnetic resonance angiography, SNR: signal to noise ratio, ECV: extra-cellular volume fraction.

Fig. 2 Interpretation algorithm for incorporating delayed enhancement-cardiac magnetic resonance imaging (DE-CMR) with stress and rest perfusion magnetic resonance imaging (MRI) for the detection of coronary disease. A: Schema of the interpretation algorithm. 1) Positive DE-CMR study: hyperenhanced myocardium consistent with a prior myocardial infarction (MI) is detected. Does not include isolated midwall or epicardial hyperenhancement which can occur in nonischemic disorders. 2) Standard negative stress study: no perfusion defects at stress or rest. 3) Standard positive stress study: perfusion defects are present with adenosine that are absent or reduced at rest. 4) Artifactual perfusion defect: matched stress and rest perfusion defects without evidence of prior MI on DE-CMR. B: Patient examples. Top row: patient with a positive DE-CMR study demonstrating an infarct in the inferolateral wall (red arrows) although perfusion-MRI is negative. The interpretation algorithm classifies this patient as positive for coronary artery disease (CAD). Coronary angiography verified disease in a circumflex marginal artery. Middle row: patient with a negative DE-CMR study but with a prominent reversible defect in the anteroseptal wall on perfusion-MRI (red arrows). The interpretation algorithm classifies this patient as positive for CAD. Coronary angiography demonstrated a proximal 95% LAD stenosis. Bottom row: patient with a matched stress-rest perfusion defect (blue arrows) but without evidence of prior MI on DE-CMR. The interpretation algorithm classifies the perfusion defects as artifactual. Coronary angiography demonstrated normal coronary arteries. Adapted from Klem et al. J Am Coll Cardiol 2006;47:1630-8, with permission of Elsevier.14) LCX: left circumflex artery, LAD: left anterior descending.

Fig. 3 Cine and delayed-enhancement images in a patient without signs or symptoms of coronary artery disease who was believed to have a structurally normal heart. Images demonstrate a focal subendocardial infarct (arrows) with normal left ventricular size and systolic function. CMR: cardiac magnetic resonance imaging, DE: delayed enhancement.
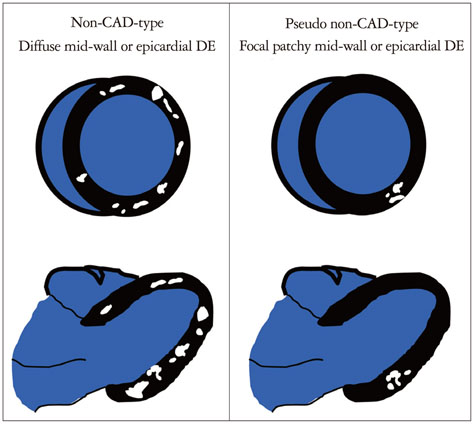
Fig. 4 The cartoon schematic on the left demonstrates multiple islands of hyperenhancement in a diffuse, near global pattern, which is classic for particular types of viral myocarditis. In other words, the correct interpretation of this pattern would be "non-CAD-type". In contrast, it would be incorrect to judge the pattern on the right, which shows only a few "dots" of hyperenhancement in a limited, focal territory, as non-CAD-type. CAD: coronary artery disease, DE: delayed enhancement.
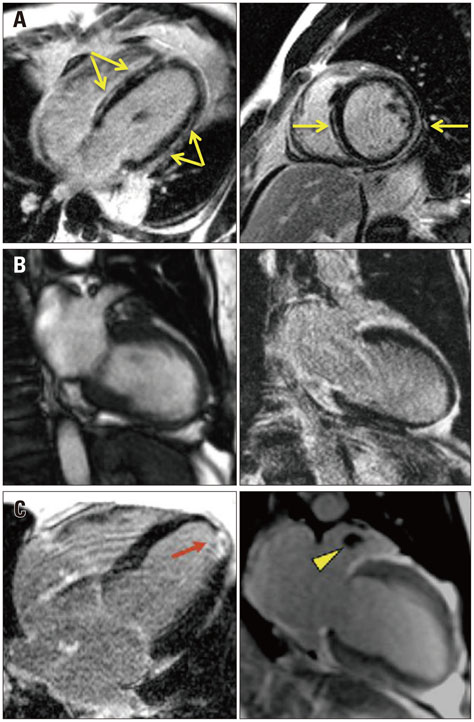
Fig. 5 Typical delayed enhancement-cardiac magnetic resonance (DE-CMR) images from 3 patients with chest discomfort, ST-segment elevation, positive troponins, and normal invasive coronary angiograms. A: Linear, epicardial hyperenhancement (yellow arrows) is present and is indicative of myocarditis. B: Cine and DE images of a patient with sudden emotional stress and apical ballooning; the absence of hyper-enhancement is consistent with Takotsubo cardiomyopathy. C: Focal but transmural hyperenhancement (red arrow) involving the lateral apex is present and indicative of myocardial infarction (MI) because of temporary occlusion of a small diagonal branch off the distal left anterior descending coronary artery. DE-CMR with a long inversion time (600 ms) shows a thrombus (yellow arrowhead) in the left atrial appendage, suggesting that an embolus led to the MI.
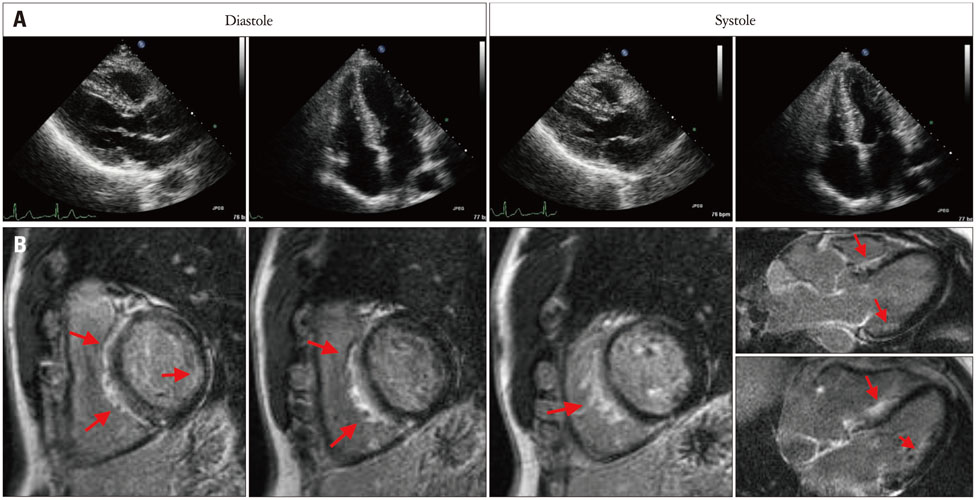
Fig. 6 A 57-year-old patient with paroxysmal atrial fibrillation undergoing cardiac magnetic resonance imaging (CMR) prior to radiofrequency ablation procedure. A: Echocardiogram demonstrated normal left ventricular (LV) size and function and only mild LV wall hypertrophy. B: Delayed enhancement-CMR images demonstrated widespread hyperenhancement (arrows) primarily in a non-coronary artery disease-type pattern, which suggested an infiltrative process.
Reference
-
1. Kim HW, Farzaneh-Far A, Kim RJ. Cardiovascular magnetic resonance in patients with myocardial infarction: current and emerging applications. J Am Coll Cardiol. 2009; 55:1–16.2. Kim HW, Klem I, Shah DJ, Wu E, Meyers SN, Parker MA, Crowley AL, Bonow RO, Judd RM, Kim RJ. Unrecognized non-Q-wave myocardial infarction: prevalence and prognostic significance in patients with suspected coronary disease. PLoS Med. 2009; 6:e1000057.3. Shah R, Heydari B, Coelho-Filho O, Murthy VL, Abbasi S, Feng JH, Pencina M, Neilan TG, Meadows JL, Francis S, Blankstein R, Steigner M, di Carli M, Jerosch-Herold M, Kwong RY. Stress cardiac magnetic resonance imaging provides effective cardiac risk reclassification in patients with known or suspected stable coronary artery disease. Circulation. 2013; 128:605–614.4. Kramer CM, Barkhausen J, Flamm SD, Kim RJ, Nagel E. Society for Cardiovascular Magnetic Resonance Board of Trustees Task Force on Standardized Protocols. Standardized cardiovascular magnetic resonance (CMR) protocols 2013 update. J Cardiovasc Magn Reson. 2013; 15:91.5. Grothues F, Braun-Dullaeus R. Serial assessment of ventricular morphology and function. Heart Fail Clin. 2009; 5:301–314. v6. Gerber BL, Raman SV, Nayak K, Epstein FH, Ferreira P, Axel L, Kraitchman DL. Myocardial first-pass perfusion cardiovascular magnetic resonance: history, theory, and current state of the art. J Cardiovasc Magn Reson. 2008; 10:18.7. Sievers B, Elliott MD, Hurwitz LM, Albert TS, Klem I, Rehwald WG, Parker MA, Judd RM, Kim RJ. Rapid detection of myocardial infarction by subsecond, free-breathing delayed contrast-enhancement cardiovascular magnetic resonance. Circulation. 2007; 115:236–244.8. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O, Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999; 100:1992–2002.9. Wagner A, Mahrholdt H, Holly TA, Elliott MD, Regenfus M, Parker M, Klocke FJ, Bonow RO, Kim RJ, Judd RM. Contrast-enhanced MRI and routine single photon emission computed tomography (SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: an imaging study. Lancet. 2003; 361:374–379.10. Ricciardi MJ, Wu E, Davidson CJ, Choi KM, Klocke FJ, Bonow RO, Judd RM, Kim RJ. Visualization of discrete microinfarction after percutaneous coronary intervention associated with mild creatine kinase-MB elevation. Circulation. 2001; 103:2780–2783.11. White SK, Sado DM, Flett AS, Moon JC. Characterising the myocardial interstitial space: the clinical relevance of non-invasive imaging. Heart. 2012; 98:773–779.12. Banypersad SM, Sado DM, Flett AS, Gibbs SD, Pinney JH, Maestrini V, Cox AT, Fontana M, Whelan CJ, Wechalekar AD, Hawkins PN, Moon JC. Quantification of myocardial extracellular volume fraction in systemic AL amyloidosis: an equilibrium contrast cardiovascular magnetic resonance study. Circ Cardiovasc Imaging. 2013; 6:34–39.13. Sado DM, White SK, Piechnik SK, Banypersad SM, Treibel T, Captur G, Fontana M, Maestrini V, Flett AS, Robson MD, Lachmann RH, Murphy E, Mehta A, Hughes D, Neubauer S, Elliott PM, Moon JC. Identification and assessment of Anderson-Fabry disease by cardiovascular magnetic resonance noncontrast myocardial T1 mapping. Circ Cardiovasc Imaging. 2013; 6:392–398.14. Klem I, Heitner JF, Shah DJ, Sketch MH Jr, Behar V, Weinsaft J, Cawley P, Parker M, Elliott M, Judd RM, Kim RJ. Improved detection of coronary artery disease by stress perfusion cardiovascular magnetic resonance with the use of delayed enhancement infarction imaging. J Am Coll Cardiol. 2006; 47:1630–1638.15. Kim RJ, Albert TS, Wible JH, Elliott MD, Allen JC, Lee JC, Parker M, Napoli A, Judd RM. Gadoversetamide Myocardial Infarction Imaging Investigators. Performance of delayed-enhancement magnetic resonance imaging with gadoversetamide contrast for the detection and assessment of myocardial infarction: an international, multicenter, double-blinded, randomized trial. Circulation. 2008; 117:629–637.16. Kwong RY, Schussheim AE, Rekhraj S, Aletras AH, Geller N, Davis J, Christian TF, Balaban RS, Arai AE. Detecting acute coronary syndrome in the emergency department with cardiac magnetic resonance imaging. Circulation. 2003; 107:531–537.17. Jaarsma C, Leiner T, Bekkers SC, Crijns HJ, Wildberger JE, Nagel E, Nelemans PJ, Schalla S. Diagnostic performance of noninvasive myocardial perfusion imaging using single-photon emission computed tomography, cardiac magnetic resonance, and positron emission tomography imaging for the detection of obstructive coronary artery disease: a meta-analysis. J Am Coll Cardiol. 2012; 59:1719–1728.18. Greenwood JP, Maredia N, Younger JF, Brown JM, Nixon J, Everett CC, Bijsterveld P, Ridgway JP, Radjenovic A, Dickinson CJ, Ball SG, Plein S. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial. Lancet. 2012; 379:453–460.19. Kato S, Kitagawa K, Ishida N, Ishida M, Nagata M, Ichikawa Y, Katahira K, Matsumoto Y, Seo K, Ochiai R, Kobayashi Y, Sakuma H. Assessment of coronary artery disease using magnetic resonance coronary angiography: a national multicenter trial. J Am Coll Cardiol. 2010; 56:983–991.20. Yang Q, Li K, Liu X, Du X, Bi X, Huang F, Jerecic R, Liu Z, An J, Xu D, Zheng H, Fan Z, Li D. 3.0T whole-heart coronary magnetic resonance angiography performed with 32-channel cardiac coils: a single-center experience. Circ Cardiovasc Imaging. 2012; 5:573–579.21. Senthilkumar A, Majmudar MD, Shenoy C, Kim HW, Kim RJ. Identifying the etiology: a systematic approach using delayed-enhancement cardiovascular magnetic resonance. Heart Fail Clin. 2009; 5:349–367. vi22. Shah DJ, Kim HW, Kim RJ. Evaluation of ischemic heart disease. Heart Fail Clin. 2009; 5:315–332. v
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac MR Assessment of Coronary Arteries
- Additive Role of Coronary Magnetic Resonance Angiography for the Evaluation of Coronary Artery Disease
- Anomalous Origin of the Coronary Artery from the Pulmonary Artery in Children and Adults: A Pictorial Review of Cardiac Imaging Findings
- Assessment of Myocardial Ischemia Using Stress Perfusion Cardiovascular Magnetic Resonance
- Fractional Flow Reserve: The Past, Present and Future
