A Case of Autoimmune Hemolytic Anemia Treated with Rituximab in a Child
- Affiliations
-
- 1Department of Pediatrics, Kyungpook National University School of Medicine, Daegu, Korea. kslee@knu.ac.kr
- KMID: 2305222
- DOI: http://doi.org/10.5045/kjh.2006.41.4.321
Abstract
- Autoimmune hemolytic anemia (AIHA) in children usually responds well to short-term steroid therapy. However, in some cases, AIHA requires prolonged immunosuppressive therapy, with the subsequent development of severe side effects. Compared with previous conventional immunosuppressive therapy, rituximab, an anti-CD20 chimeric monoclonal antibody, shows good therapeutic efficacy and safety in the treatment of autoimmune disorders. Herein, the case of a 13-year-old male patient, who showed a remarkable and durable response to rituximab, at a dose of 375mg/m2, is reported. Before this trial, he had been a hepatitis B carrier and steroid dependent AIHA for 4 years, with a cushingoid facial appearance and growth retardation. After 10 months, he experienced a recurrence of hemolysis, which was successfully retreated, and was then taken off the steroid therapy. The therapy was well tolerated, without serious complications. It is suggested that rituximab could be a new option in the treatment of steroid-dependent AIHA. Therefore, long-term follow-up and studies of the risk factors of a relapse are warranted.
Keyword
MeSH Terms
Figure
-
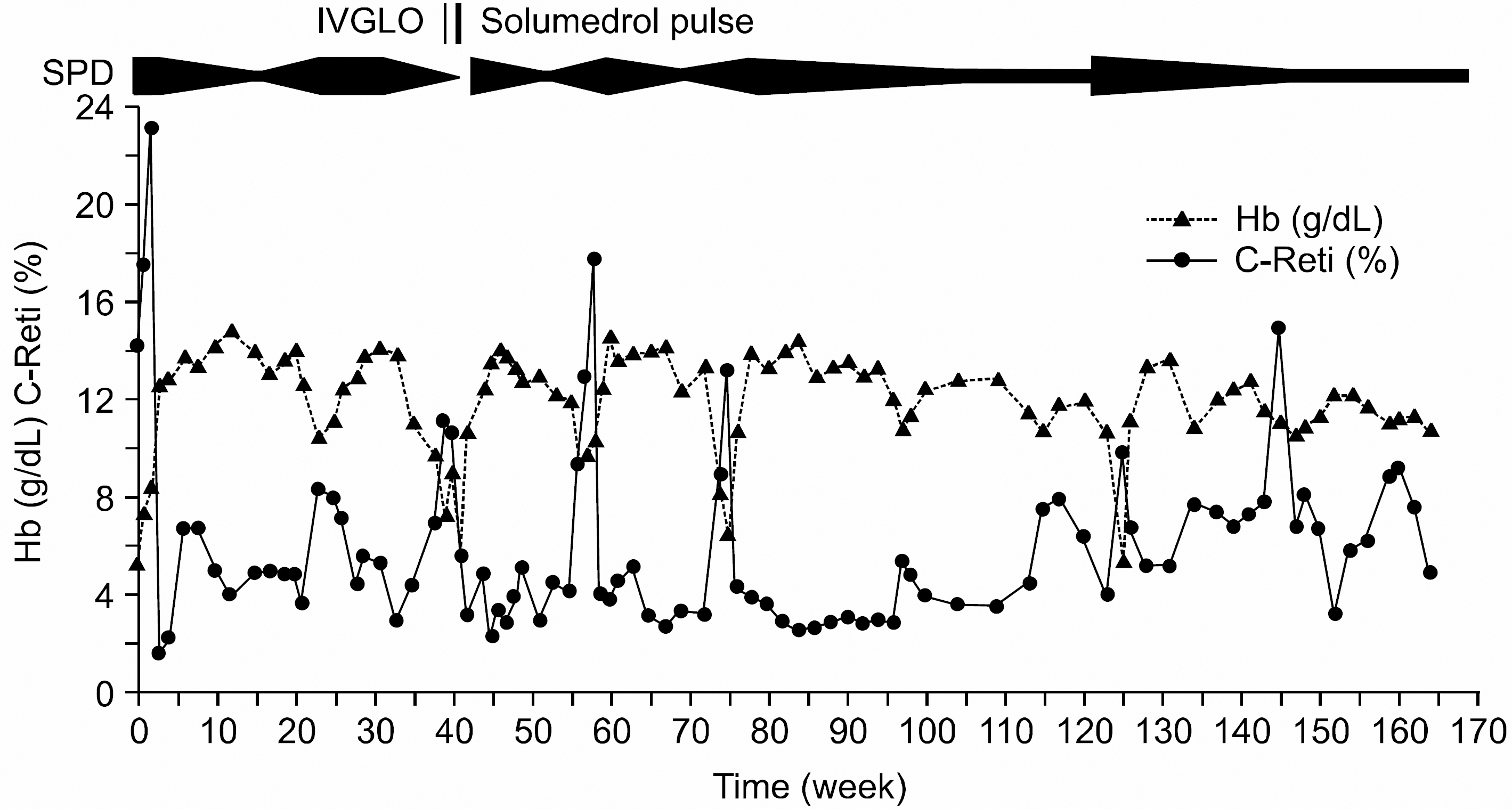
Fig. 1 The response of hemoglobin and corrected reticulocyte count before rituximab treatment. SPD, prednisolone; IVGLO, intravenous immunoglobulin O; So-lumedrol pulse, high dose methylprednisolone; C-Reti, corrected reticulocyte count.
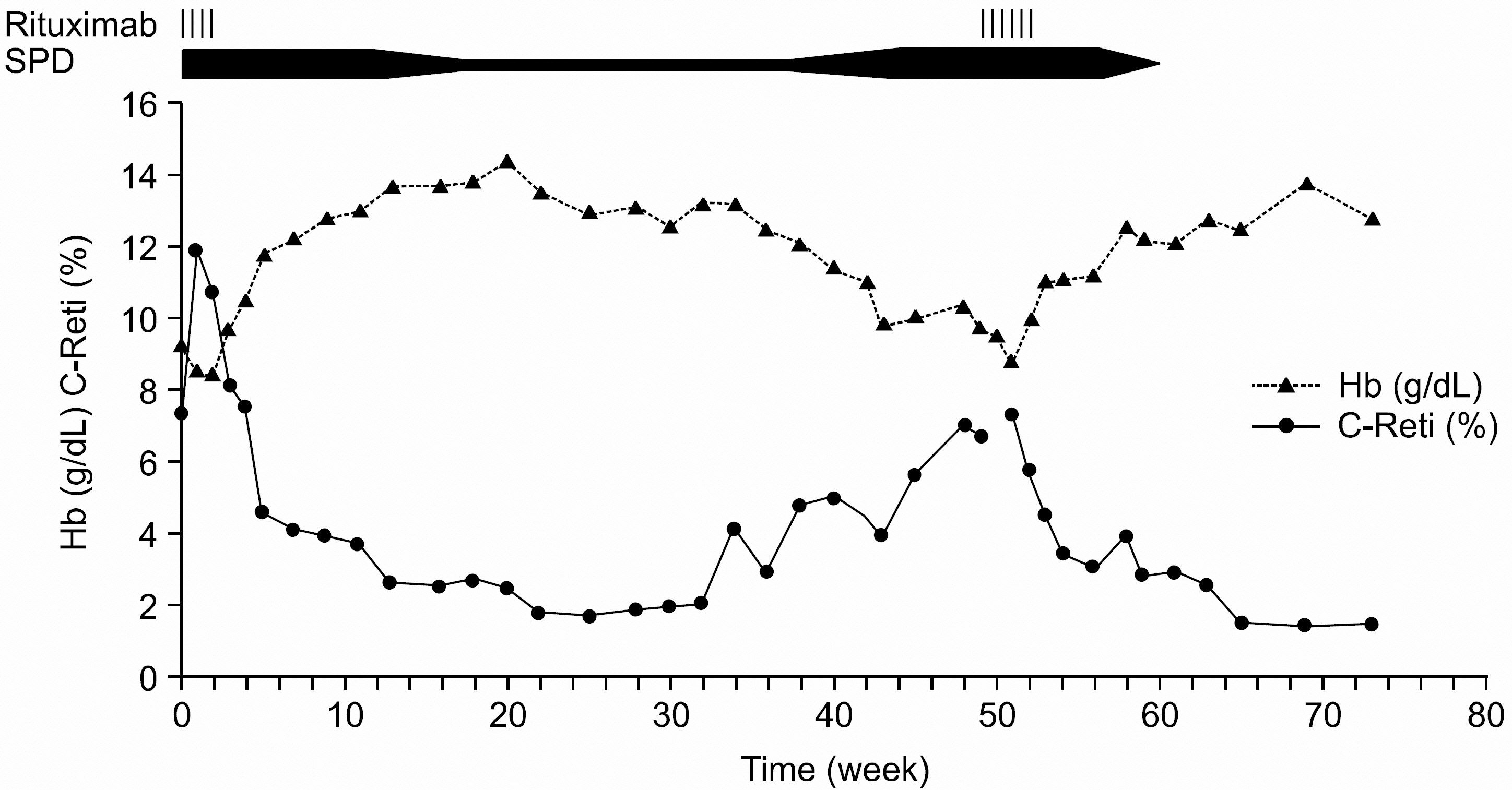
Fig. 2 The hemoglobin and corrected reticulocyte count after rituximab treatment.
Cited by 3 articles
-
Steroid-refractory Autoimmune Hemolytic Anemia Following Unrelated Allogeneic Peripheral Blood Stem Cell Transplantation
Seong-Rye Seo, Yeo-Kyeoung Kim, Soo-Young Bae, Joo-Young Yoon, Seong-Wook Lim, Jae-Sook Ahn, Deok-Hwan Yang, Sang-Hee Cho, Je-Jung Lee, Ik-Joo Chung, Hyeoung-Joon Kim
Chonnam Med J. 2008;44(3):184-187. doi: 10.4068/cmj.2008.44.3.184.Delayed and Long-term Remission of Refractory Hemolytic Anemia in a Child with Systemic Lupus Erythematosus Treated with Rituximab
Ju Hwan Park, Jae Wook Im, Hong Kil Jun, Hae Min Park, Seung Won Choi, Sang Kyu Park, Ji Seon Oh
J Rheum Dis. 2014;21(4):196-200. doi: 10.4078/jrd.2014.21.4.196.A Case of Autoimmune Hemolytic Anemia Complicating Hematopoietic Cell Transplantation
Hyojin Chae, Yonggoo Kim, Myungshin Kim, Jihyang Lim, Kyungja Han, Seok Goo Cho, Jong-Wook Lee
Korean J Lab Med. 2008;28(1):64-69. doi: 10.3343/kjlm.2008.28.1.64.
Reference
-
1). George BS. Hemolytic anemias resulting from extracellular factors. Behrman RE, Kliegman RM, Jenson HB, editors. Nelson textbook of pediatrics. 17th ed.Philadelphia: WB Saunders Co;2004. p. 1638–40.2). Reff ME., Carner K., Chambers KS, et al. Depletion of B cells in vivo by a chimeric mouse human monoclonal antibody to CD20. Blood. 1994. 83:435–45.
Article3). McLaughlin P., Grillo-Lopez AJ., Link BK, et al. Rituximab chimeric anti-CD20 monoclonal antibody therapy for relapsed indolent lymphoma: half of patients respond to a four-dose treatment program. J Clin Oncol. 1998. 16:2825–33.
Article4). Yang DH., Lee JJ., Kim YK, et al. The clinical efficacy of R-CHOP chemotherapy in patients with previously untreated diffuse large B-cell lymphoma. Korean J Hematol. 2004. 39:59–65.5). Lee EJ., Kueck B. Rituxan in the treatment of cold agglutinin disease. Blood. 1998. 92:3490–1.
Article6). Quartier P., Brethon B., Philippet P., Landman-Parker J., Le Deist F., Fischer A. Treatment of childhood autoimmune haemolytic anaemia with rituximab. Lancet. 2001. 358:1511–3.
Article7). Zecca M., Nobili B., Ramenghi U, et al. Rituximab for the treatment of refractory autoimmune hemolytic anemia in children. Blood. 2003. 101:3857–61.
Article8). Ramanathan S., Koutts J., Hertzberg MS. Two cases of refractory warm autoimmune hemolytic anemia treated with rituximab. Am J Hematol. 2005. 78:123–6.
Article9). Wang J., Wiley JM., Luddy R., Greenberg J., Feuer-stein MA., Bussel JB. Chronic immune thrombocytopenic purpura in children: assessment of rituixmab treatment. J Pediatr. 2005. 146:217–21.10). Park SJ., Han CW. The long term remission effect of rituximab in two patients with autoimmune-associated cytopenias that were refractory to standard treatments. Korean J Hematol. 2005. 40:101–5.
Article11). Park US., Choi CB., Kim JS, et al. A case of post-transplantation lymphoproliferative disease developed in renal transplant recipient and treated with rituximab. Korean J Med. 2004. 67:94–9.12). Heisel MA., Ortega JA. Factors influencing prognosis in childhood autoimmune hemolytic anemia. Am J Pediatr Hematol Oncol. 1983. 5:147–52.13). Hamaki T., Kami M., Kusumi E, et al. Prophylaxis of hepatitis B reactivation using lamivudine in a patient receiving rituximab. Am J Hematol. 2001. 68:292–4.
Article14). Tsutsumi Y., Tanaka J., Kawamura T, et al. Possible efficacy of lamivudine treatment to prevent hepatitis B virus reactivation due to rituximab therapy in a patient with non-hodgkin's lymphoma. Ann Hematol. 2004. 83:58–60.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Delayed and Long-term Remission of Refractory Hemolytic Anemia in a Child with Systemic Lupus Erythematosus Treated with Rituximab
- Quetiapine Induced Autoimmune Hemolytic Anemia in a Child Patient: A Case Report
- Evans syndrome following long-standing Hashimoto's thyroiditis and successful treatment with rituximab
- Successful Treatment of a Korean Infant with Giant Cell Hepatitis with Autoimmune Hemolytic Anemia Using Rituximab
- Two Cases of Autoimmune Hemolytic Anemic
