Korean Circ J.
2009 Feb;39(2):79-81. 10.4070/kcj.2009.39.2.79.
A Case of Aspergillus Endocarditis Presenting as Endophthalmitis
- Affiliations
-
- 1Department of Cardiology, Catholic University of Daegu, School of Medicine, Daegu, Korea. jychoi@cu.ac.kr
- 2Department of Pathology, Catholic University of Daegu, School of Medicine, Daegu, Korea.
- KMID: 2297954
- DOI: http://doi.org/10.4070/kcj.2009.39.2.79
Abstract
- Aspergillus endocarditis is an uncommon, but often fatal, disease that usually occurs in patients who have had prior cardiac surgery. Endophthalmitis is a very rare complication of infective endocarditis, especially at presentation. We report a case of Aspergillus endocarditis in a 68-year-old woman who presented with endophthalmitis.
Keyword
Figure
-
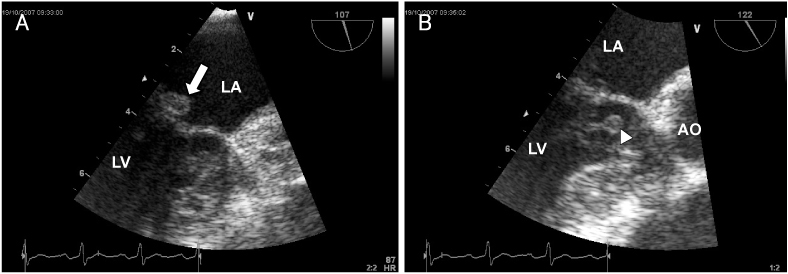
Fig. 1 Transesophageal echocardiography findings. Multiple vegetations are attached to the posterior mitral valve (A: white arrow) and chordae of the anterior mitral leaflet (B: arrow head). LA: left atrium, LV: left ventricle, AO: aorta.

Fig. 2 Magnetic resonance imaging (MRI) of the brain. There is acute intracerebral hemorrhage in the right temporoparietal lobe, with intraventricular hemorrhage.

Fig. 3 3D-computed tomographic angiography of brain. There is a fusiform aneurysm in the right middle cerebral artery (arrow).
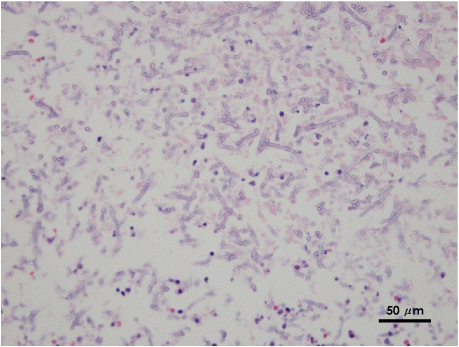
Fig. 4 Pathologic findings of aspirated cerebral aneurysm tissue. There are many fungal hyphae against a necrotic background. Branching hyphae with acute angles are occasionally noted, as well (H & E, ×400).
Reference
-
1. Baek JS, Bang JS, Bae EJ, et al. Current characteristics of infective endocarditis with congenital heart disease: a retrospective survey of 121 cases between 1985 and 2006. Korean Circ J. 2007. 37:635–640.2. Ahn S, Lee MH, Pyun WB, Kim SS. Clinical observation of infective endocarditis. Korean Circ J. 2000. 30:166–173.3. Ellis ME, Al-Abdely H, Sandridge A, Greer W, Ventura W. Fungal endocarditis: evidence in the world literature, 1965-1995. Clin Infect Dis. 2001. 32:50–62.4. El-Hamamsy I, Dürrleman N, Stevens LM, Perrault LP, Carrier M. Aspergillus endocarditis after cardiac surgery. Ann Thorac Surg. 2005. 80:359–364.5. Gumbo T, Taege AJ, Mawhorter S, et al. Aspergillus valve endocarditis in patient without prior cardiac surgery. Medicine. 2000. 79:261–268.6. Pras E, Rubowitz A, Ferencz JR, Raz J, Rotenstereich Y, Assia EI. Endogenous endophthalmitis as the leading sign of endocarditis. Ann Ophthalmol. 2001. 33:148–150.7. Maliaga A, Mintzias D, Zigouris N, Rigatou IK, Skoutelis A. Bacterial endocarditis with dual presentation as endophthalmitis and glomerulonephritis. Eur J Intern Med. 2006. 17:125–126.8. Pierrotti LC, Baddour LM. Fungal endocarditis, 1995-2000. Chest. 2002. 122:302–310.9. Rubinstein E, Lang R. Fungal endocarditis. Eur Heart J. 1995. 16 Suppl B:84–89.10. Chee SP, Jap A. Endogenous endophthalmitis. Curr Opin Ophthalmol. 2001. 12:464–470.11. Greenwald MJ, Wohl LG, Sell CH. Metastatic bacterial endophthalmitis: a contemporary reappraisal. Surv Ophthalmol. 1986. 31:81–101.12. Lemley CA, Han DP. Endophthalmitis: a review of current evaluation and management. Retina. 2007. 27:662–680.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Group G Streptococcal Endocarditis Associated with Bilateral Endogenous Endophthalmitis
- Infective Endocarditis Presenting as Endogenous Endophthalmitis Secondary to Streptococcus agalactiae in a Healthy Adult: Case Report and Literature Review
- Cerebral Basilar Artery Mycotic Aneurysm Associated With Aspergillus Endogenous Endophthalmitis
- Two Cases of Aspergillus Endocarditis in Patients with Acute Lymphoblastic Leukemia
- Endophthalmitis: Riview of the Literature and Report of Three Cases
