Reverse Controlled Antegrade and Retrograde Subintimal Tracking in Chronic Total Occlusion of Right Coronary Artery
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Gwangju Veterans Hospital, Gwangju, Korea. h96241085@hanmail.net
- 2Division of Cardiology, Department of Internal Medicine, Kyung Hee University College of Medicine, Seoul, Korea.
- KMID: 2297894
- DOI: http://doi.org/10.4070/kcj.2012.42.9.625
Abstract
- Passage failure of guidewire is still remained most common reason for percutaneous coronary intervention (PCI) failure in chronic total occlusion (CTO). Intravascular ultrasound study (IVUS) and cardiac CT angiography can help identify features that most influence current success rates of PCI. We report our experience using the reverse controlled antegrade and retrograde subintimal tracking technique under the aid of IVUS, cardiac CT angiography for an ambiguous CTO of proximal right coronary artery.
Keyword
MeSH Terms
Figure
-

Fig. 1 Images of pre-interventional coronary angiography. Chronic total occlusion of the proximal right coronary artery (A) with grade 3 collateral flow from the left anterior descending artery (B) revealed by coronary angiography. A small vessel of the proximal portion of right coronary artery (arrow) appears to be the conus branch (A).
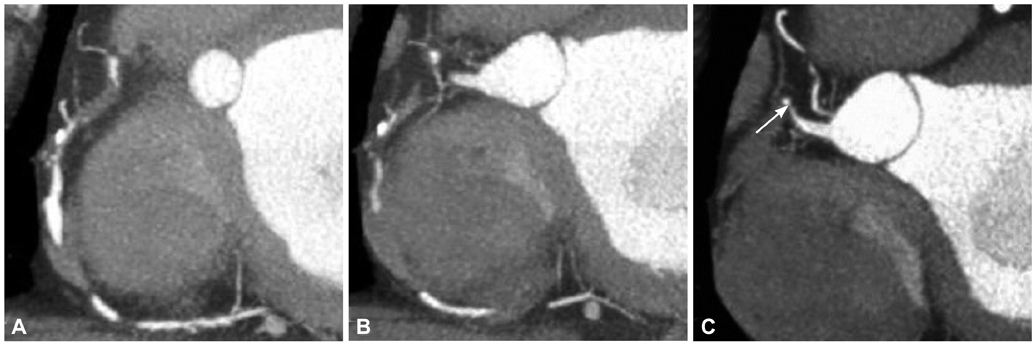
Fig. 2 Computed tomography (CT) coronary angiography of chronic total occlusion. Segmental calcified and soft plaques of proximal right coronary artery (RCA) with chronic total occlusion (CTO) were detected in cardiac CT angiography (A and B). A small branch of the proximal portion of the RCA (arrow) was considered a tapered-type CTO lesion rather than a conus branch by coronary angiography and intravascular ultrasound (C).

Fig. 3 "Reverse CART technique". The wires pass via septal branch to mid-distal right coronary artery (RCA) via retrograde approach (A and B). The percutaneous transluminal coronary angioplasty for proximal RCA and mid RCA was performed. In addition, 3 drug-eluting stents were deployed (C). Final angiographic result showed good distal flow without residual stenosis (D). CART: controlled antegrade and retrograde subintimal tracking.
Reference
-
1. Hoye A, van Domburg RT, Sonnenschein K, Serruys PW. Percutaneous coronary intervention for chronic total occlusions: the Thoraxcenter experience 1992-2002. Eur Heart J. 2005. 26:2630–2636.2. Ishizaka N, Issiki T, Saeki F, et al. Angiographic follow-up after successful percutaneous coronary angioplasty for chronic total coronary occlusion: experience in 110 consecutive patients. Am Heart J. 1994. 127:8–12.3. Olivari Z, Rubartelli P, Piscione F, et al. Immediate results and one-year clinical outcome after percutaneous coronary interventions in chronic total occlusions: data from a multicenter, prospective, observational study (TOAST-GISE). J Am Coll Cardiol. 2003. 41:1672–1678.4. Suero JA, Marso SP, Jones PG, et al. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries: a 20-year experience. J Am Coll Cardiol. 2001. 38:409–414.5. Prasad A, Rihal CS, Lennon RJ, Wiste HJ, Singh M, Holmes DR Jr. Trends in outcomes after percutaneous coronary intervention for chronic total occlusions: a 25-year experience from the Mayo Clinic. J Am Coll Cardiol. 2007. 49:1611–1618.6. Kinoshita I, Katoh O, Nariyama J, et al. Coronary angioplasty of chronic total occlusions with bridging collateral vessels: immediate and follow-up outcome from a large single-center experience. J Am Coll Cardiol. 1995. 26:409–415.7. Park Y, Park HS, Jang GL, et al. Intravascular ultrasound guided recanalization of stumpless chronic total occlusion. Int J Cardiol. 2011. 148:174–178.8. Hoe J. CT coronary angiography of chronic total occlusions of the coronary arteries: how to recognize and evaluate and usefulness for planning percutaneous coronary interventions. Int J Cardiovasc Imaging. 2009. 25:Suppl 1. 43–54.9. Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv. 2008. 71:8–19.10. Rathore S, Katoh O, Tuschikane E, Oida A, Suzuki T, Takase S. A novel modification of the retrograde approach for the recanalization of chronic total occlusion of the coronary arteries intravascular ultrasound-guided reverse controlled antegrade and retrograde tracking. JACC Cardiovasc Interv. 2010. 3:155–164.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Iteration of Reverse Controlled Antegrade and Retrograde Tracking for Coronary Chronic Total Occlusion Intervention: a Current Appraisal
- Successful Recanalization of a Long Superficial Femoral Artery Occlusion by Retrograde Subintimal Angioplasty After a Failed Antegrade Subintimal Approach
- Strategies for Successful Percutaneous Revascularization of Chronic Total Occlusion of the Femoropopliteal Arteries When the Antegrade Passage of a Guide Wire Fails
- Subintimal Tracking and Re-entry (STAR) Technique with Contrast Guidance for Chronic Total Occlusion: Experience with 4 Cases
- Recanalization of a Coronary Chronic Total Occlusion by a Retrograde Approach Using Ipsilateral Double Guiding Catheters
