J Rhinol.
2015 May;22(1):6-10. 10.18787/jr.2015.22.1.6.
Prospective Study on the Characteristics and Postoperative Improvement of Rhinogenic Headache
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Seoul National University College of Medicine, Seoul, Korea. dongkim@snu.ac.kr
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Chosun University College of Medicine, Gwang-ju, Korea.
- 3Department of Otorhinolaryngology-Head and Neck Surgery, Pusan National University College of Medicine, Pusan, Korea.
- 4Department of Otorhinolaryngology-Head and Neck Surgery, Soon Chun Hyang University College of Medicine, Seoul, Korea.
- 5Research Center for Sensory Organs, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2297548
- DOI: http://doi.org/10.18787/jr.2015.22.1.6
Abstract
- BACKGROUND AND OBJECTIVES
Headache secondary to sinonasal disease can improve after surgery, but few prospective studies have investigated this outcome. We aimed to evaluate the characteristics of headaches, such as clinical features, underlying disease, and postoperative improvement in patients who underwent nasal surgery, and to identify the characteristics that reliably predict rhinogenic headache. MATERIALS AND METHOD: Of 356 patients who underwent nasal surgery between March and December 2009, 41 patients with headaches were enrolled in this prospective study. Clinical features of headache, such as onset, time of day, duration, frequency, nature, side and location, existence of aura, aggravating and relieving factors and accompanying nasal symptoms, underlying diseases, endoscopic findings, and computed tomography scans of the paranasal sinuses were evaluated. Headache intensity was graded based on a 10-point visual analog scale (VAS) pre- and post-operatively.
RESULTS
The most common characteristics of rhinogenic headache included a stabbing or squeezing nature, frontal area location, accompanying nasal obstruction or rhinorrhea, and underlying sinusitis or septal deviation. The subjective intensity of the headache, measured using the VAS score, improved in 80% (33/41) of the patients after surgery.
CONCLUSION
Nasal surgery should be considered when rhinogenic headache is suspected and there are definite nasal pathologies.
MeSH Terms
Figure
-
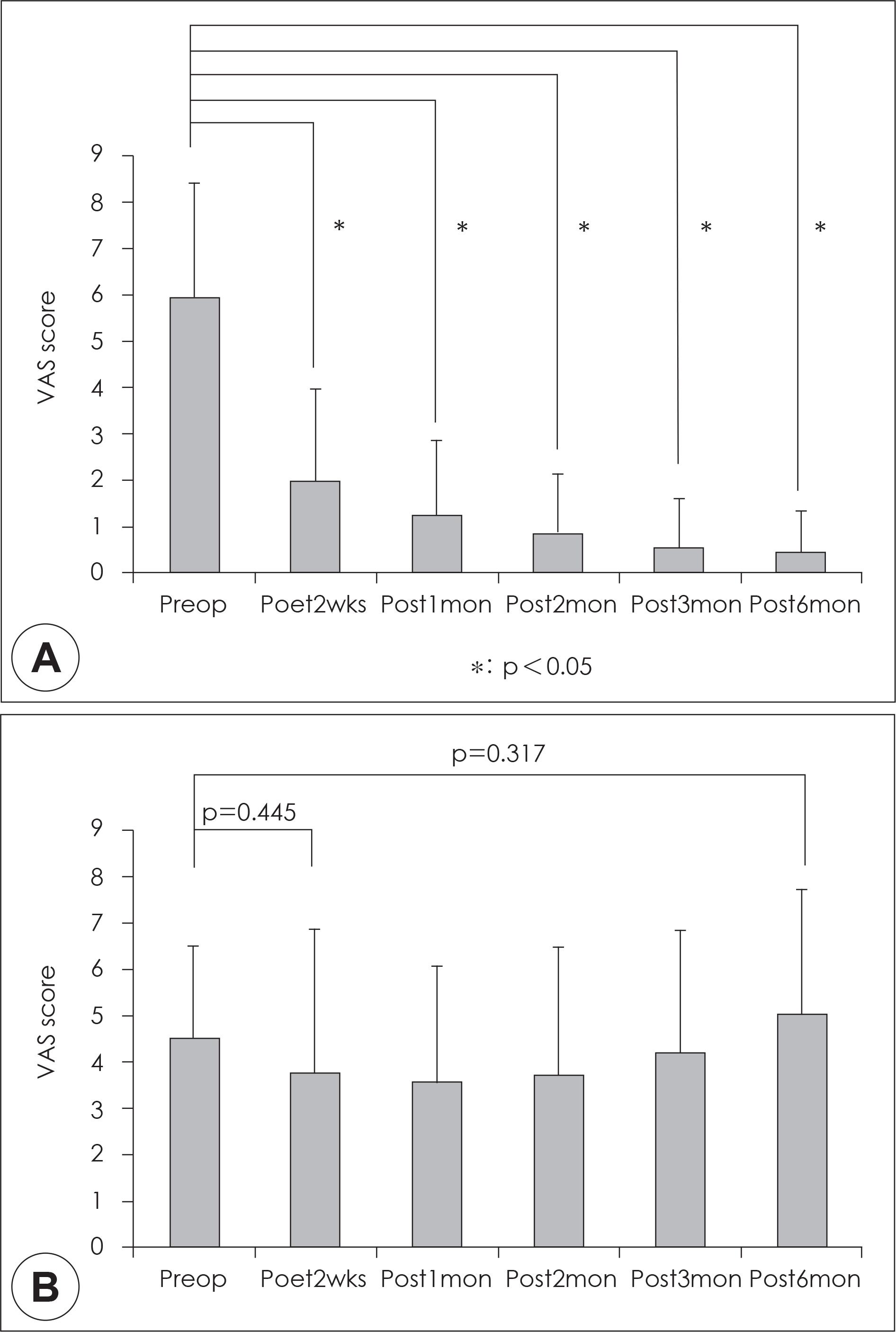
Fig. 1. Pre-and post-operative visual analog scale score for headache in the resolved and improved groups (A) and in the no-change and worsened groups (B). *: p<0.05. VAS: visual analog scale, Preop: Preoperative, Post: Postoperative, wks: weeks, mon: months.
Reference
-
References
1). Cady RK, Dodick DW, Levine HL, Schreiber CP, Eross EJ, Setzen M, et al. Sinus headache: A neurology, otolaryngology, allergy, and primary care consensus on diagnosis and treatment. Mayo Clin Proc. 2005; 80:908–16.
Article2). Chung SK. Headache and facial pain related to the paranasal sinuses. J Rhinol. 2012; 19:83–6.3). Mariotti LJ, Setliff RC, Ghaderi M, Voth S. Patient history and CT findings in predicting surgical outcomes for patients with rhinogenic headache. Ear Nose Throat J. 2009; 88:926–9.
Article4). Lund VJ, Mackay IS. Staging in rhinosinusitus. Rhinology 1993;31:. 183–4.5). Blumenthal HJ. Headaches and sinus disease. Headache 2001;41: 883–8.6). Mohebbi A, Memari F, Mohebbi S. Endonasal endoscopic management of contact point headache and diagnostic criteria. Headache. 2010; 50:242–8.
Article7). Schonsted-Madsen U, Stoksted P, Christensen PH, Koch-Henriksen N. Chronic headache related to nasal obstruction. J Laryngol Otol. 1986; 100:165–70.8). Low WK, Willatt DJ. Headaches associated with nasal obstruction due to deviated nasal septum. Headache. 1995; 35:404–6.
Article9). Parsons DS, Batra PS. Functional endoscopic sinus surgical outcomes for contact point headaches. Laryngoscope. 1998; 108:696–702.
Article10). Ramadan HH. Nonsurgical versus endoscopic sinonasal surgery for rhinogenic headache. Am J Rhinol. 1999; 13:455–7.
Article11). Stammberger H, Wolf G. Headaches and sinus disease: the endoscopic approach. Ann Otol Rhinol Laryngol Suppl. 1988; 134:3–23.
Article12). Clerico DM, Evan K, Montgomery L, Lanza DC, Grabo D. Endoscopic sinonasal surgery in the management of primary headaches. Rhinology. 1997; 35:98–102.13). Tosun F, Gerek M, Ozkaptan Y. Nasal surgery for contact point headaches. Headache. 2000; 40:237–40.
Article14). Welge-Luessen A, Hauser R, Schmid N, Kappos L, Probst R. Endonasal surgery for contact point headaches: A 10-year longitudinal study. Laryngoscope. 2003; 113:2151–6.
Article15). Lee JH, Ahn TJ, Ahn SY, Bae WY. Surgical treatment of contact point headache. J Rhinol. 2010; 17:29–32.16). Mahajan CS, Kochhar AC, Gupta AK. Sinugenic headache and nasal endoscopy. Armed Forces Med J India. 2003; 59:121–4.
Article17). Tarabichi M. Characteristics of sinus-related pain. Otolaryngol Head Neck Surg. 2000; 122:842–7.
Article18). Ragab SM, Lund VJ, Scadding G. Evaluation of the medical and surgical treatment of chronic rhinosinusitis: a prospective, randomized, controlled trial. Laryngoscope. 2004; 114:923–30.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Radiofrequency Diathermy for Rhinogenic Headache
- Rhinogenic Headache: The International Classification of Headache Disorders, 3rd Edition
- A clinical study on headache in the elderly
- Headache Characteristics in Rhinologic Patients and the Role of Surgical Treatment
- Clinical Characteristics of Rhinogenic Optic Neuropathy Associated with Paranasal Sinus Disease
