The Oncologic Safety of Skin Sparing Mastectomy with or without Conservation of the Nipple-areolar Complex: 5 Years Follow up Results
- Affiliations
-
- 1Department of Surgery, Yeungnam University College of Medicine, Daegu, Korea. crystallee@medical.yu.ac.kr
- 2Department of Pathology, Yeungnam University College of Medicine, Daegu, Korea.
- KMID: 2286562
- DOI: http://doi.org/10.4048/jbc.2010.13.1.65
Abstract
- PURPOSE
Little is known about long term results of nipple-areola preserving skin-sparing mastectomy (NASSM), and there are no such reports on this from South Korea. We studied 5 years follow up results of NASSM and skin sparing mastectomy (SSM) and compared clinical outcomes between NASSM and SSM.
METHODS
Two hundred two patients who underwent SSM (69 patients) or NASSM (133 patients) from September 1996 to December 2006 were included. Frozen section analysis of retroareolar resection margin was done to make the decision on preserving or not preserving nipple-areolar complex (NAC). In the case of positive result on the frozen section, NAC was sacrificed. The local relapse (LR) rate and local relapse free survival (LFS) were analyzed for comparing between NASSM and SSM.
RESULTS
The mean age was 40.2 years (range, 24-65), the mean follow-up was 67.6 months. 52 NACs (25.7%) were involved by tumor cells. The invasion to the NAC by tumor cell was more common for invasive carcinoma with extensive intraductal component (p<0.001), central located tumor (p=0.025) and invasive carcinoma with multiplicity (p=0.001). There were 12 cases (9.0%) of local relapse in NASSM group and 4 (5.8%) in SSM group, but there was no significant correlation for the LR rate (p>0.05). Regional or distant recurrence after surgical treatment for local relapse occurred in only one SSM case. Five years LFS rate of the NASSM group was 92.1% and that of the SSM group was 95.2%. There was no significant difference for the LFS (p>0.05).
CONCLUSION
Our long term follow up study showed that NASSM and SSM are much alike for their LR rate and LFS. Even if relapse occurs in the NAC, this recurrence cannot affect the progression of relapse after adequate local treatment. Thus, NASSM is alternative method for SSM with oncological safety and better cosmetic outcome.
Keyword
MeSH Terms
Figure
-
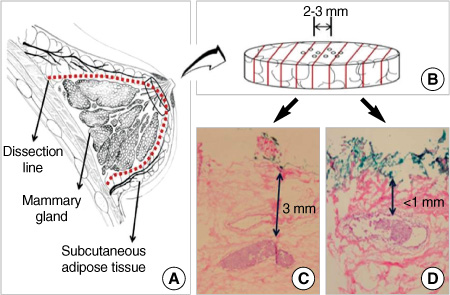
Figure 1 Dissection line of mastectomy and frozen section analysis of nipple-areolar resection margin. (A) A flap of subcutaneous adipose tissue (more than 1 cm thickness) was created and nipple-areolar resection margin was inked by blue ink and then, blue inked resection margin was sliced in 2-3 mm interval with perpendicularly 5 mm thickness.(B) In (C) case, the distance from resection margin to tumor cells was 3 mm. So, nipple-areolar complex could be preserved. But, if the distance was less than 2 mm (D), nipple-areolar complex was removed (C, D, H&E stain, ×10).
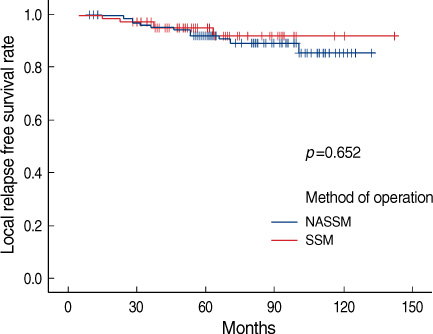
Figure 2 Local relapse free survival curves of breast cancer patients operated by NASSM vs. SSM. The curve shows that there was no significant difference in the survivals. NASSM=nipple areola preserving skin sparing mastectomy; SSM=skin sparing mastectomy.
Cited by 1 articles
-
Oncologic Outcomes after Immediate Breast Reconstruction Following Total Mastectomy in Patients with Breast Cancer: A Matched Case-Control Study
Jai Min Ryu, Hyun-June Paik, Sungmin Park, Ha Woo Yi, Seok Jin Nam, Seok Won Kim, Se Kyung Lee, Jonghan Yu, Soo Youn Bae, Jeong Eon Lee
J Breast Cancer. 2017;20(1):74-81. doi: 10.4048/jbc.2017.20.1.74.
Reference
-
1. Freeman BS. Subcutaneous mastectomy for benign breast lesions with immediate or delayed prosthetic replacement. Plast Reconstr Surg Transplant Bull. 1962. 30:676–682.
Article2. Toth BA, Lappert P. Modified skin incisions for mastectomy: the need for plastic surgical input in preoperative planning. Plast Reconstr Surg. 1991. 87:1048–1053.3. Jabor MA, Shayani P, Collins DR Jr, Karas T, Cohen BE. Nipple-areola reconstruction: satisfaction and clinical determinants. Plast Reconstr Surg. 2002. 110:457–463.
Article4. Kang SH, Lee SJ, Woo SH, Jeong JH, Seul JH. Subcutaneous mastectomy with immediate reconstruction as treatment for early breast carcinomas. J Korean Surg Soc. 1999. 57:506–513.5. Nakajima H, Imanishi N, Aiso S. Arterial anatomy of the nipple-areola complex. Plast Reconstr Surg. 1995. 96:843–845.
Article6. van Deventer PV. The blood supply to the nipple-areola complex of the human mammary gland. Aesthetic Plast Surg. 2004. 28:393–398.
Article7. Kroll SS, Schusterman MA, Tadjalli HE, Singletary SE, Ames FC. Risk of recurrence after treatment of early breast cancer with skin-sparing mastectomy. Ann Surg Oncol. 1997. 4:193–197.
Article8. Simmons RM, Fish SK, Gayle L, La Trenta GS, Swistel A, Christos P, et al. Local and distant recurrence rates in skin-sparing mastectomies compared with non-skin-sparing mastectomies. Ann Surg Oncol. 1999. 6:676–681.
Article9. Medina-Franco H, Vasconez LO, Fix RJ, Heslin MJ, Beenken SW, Bland KI, et al. Factors associated with local recurrence after skin-sparing mastectomy and immediate breast reconstruction for invasive breast cancer. Ann Surg. 2002. 235:814–819.
Article10. Wellisch DK, Schain WS, Noone RB, Little JW 3rd. The psychological contribution of nipple addition in breast reconstruction. Plast Reconstr Surg. 1987. 80:699–704.
Article11. Santini D, Taffurelli M, Gelli MC, Grassigli A, Giosa F, Marrano D, et al. Neoplastic involvement of nipple-areolar complex in invasive breast cancer. Am J Surg. 1989. 158:399–403.
Article12. Smith J, Payne WS, Carney JA. Involvement of the nipple and areola in carcinoma of the breast. Surg Gynecol Obstet. 1976. 143:546–548.13. Vlajcic Z, Zic R, Stanec S, Lambasa S, Petrovecki M, Stanec Z. Nipple-areola complex preservation: predictive factors of neoplastic nipple-areola complex invasion. Ann Plast Surg. 2005. 55:240–244.14. Wertheim U, Ozzello L. Neoplastic involvement of nipple and skin flap in carcinoma of the breast. Am J Surg Pathol. 1980. 4:543–549.
Article15. Luttges J, Kalbfleisch H, Prinz P. Nipple involvement and multicentricity in breast cancer. A study on whole organ sections. J Cancer Res Clin Oncol. 1987. 113:481–487.16. Govindarajulu S, Narreddy S, Shere MH, Ibrahim NB, Sahu AK, Cawthorn SJ. Preoperative mammotome biopsy of ducts beneath the nipple areola complex. Eur J Surg Oncol. 2006. 32:410–412.
Article17. Palmieri B, Baitchev G, Grappolini S, Costa A, Benuzzi G. Delayed nipple-sparing modified subcutaneous mastectomy: rationale and technique. Breast J. 2005. 11:173–178.
Article18. Friedman EP, Hall-Craggs MA, Mumtaz H, Schneidau A. Breast MR and the appearance of the normal and abnormal nipple. Clin Radiol. 1997. 52:854–861.
Article19. Petit JY, Veronesi U, Rey P, Rotmensz N, Botteri E, Rietjens M, et al. Nipple-sparing mastectomy: risk of nipple-areolar recurrences in a series of 579 cases. Breast Cancer Res Treat. 2009. 114:97–101.
Article20. Gerber B, Krause A, Dieterich M, Kundt G, Reimer T. The oncological safety of skin sparing mastectomy with conservation of the nipple-areola complex and autologous reconstruction: an extended follow-up study. Ann Surg. 2009. 249:461–468.
Article21. Greenway RM, Schlossberg L, Dooley WC. Fifteen-year series of skin-sparing mastectomy for stage 0 to 2 breast cancer. Am J Surg. 2005. 190:918–922.
Article22. Caruso F, Ferrara M, Castiglione G, Trombetta G, De Meo L, Catanuto G, et al. Nipple sparing subcutaneous mastectomy: sixty-six months follow-up. Eur J Surg Oncol. 2006. 32:937–940.
Article23. Can Nipple-Areola-Sparing Mastectomy Be an Alternative to Mastectomy? Over 10 Years of Follow Up At A Japanese Institution. 2008. In : 31th Annual San Antonio Breast Cancer Symposium; San Antonio: American Cancer Society.24. Benediktsson KP, Perbeck L. Survival in breast cancer after nipple-sparing subcutaneous mastectomy and immediate reconstruction with implants: a prospective trial with 13 years median follow-up in 216 patients. Eur J Surg Oncol. 2008. 34:143–148.
Article25. Barreau-Pouhaer L, Le MG, Rietjens M, Arriagada R, Contesso G, Martins R, et al. Risk factors for failure of immediate breast reconstruction with prosthesis after total mastectomy for breast cancer. Cancer. 1992. 70:1145–1151.
Article26. Victor SJ, Brown DM, Horwitz EM, Martinez AA, Kini VR, Pettinga JE, et al. Treatment outcome with radiation therapy after breast augmentation or reconstruction in patients with primary breast carcinoma. Cancer. 1998. 82:1303–1309.
Article27. Williams JK, Carlson GW, Bostwick J 3rd, Bried JT, Mackay G. The effects of radiation treatment after TRAM flap breast reconstruction. Plast Reconstr Surg. 1997. 100:1153–1160.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immediate Breast Reconstruction with TRAM Flap after Nipple-Areolar Sparing Mastectomy
- Skin - sparing Mastectomy with Circumareolar Incision and Immediate TRAM & One - stage Star Flap Nipple - areolar Complex Reconstruction
- Immediate One-Stage Breast Reconstruction Including Nipple-Areolar Complex
- Aesthetic Design of Skin-Sparing Mastectomy Incisions for Immediate Autologous Tissue Breast Reconstruction in Asian Women
- Skin Sparing Mastectomy with Circumareolar Incision and Immediate TRAM and One-Stage Star Flap Nipple-Areolar Complex Reconstruction
