Persistent Direction-Fixed Nystagmus Following Canalith Repositioning Maneuver for Horizontal Canal BPPV: A Case of Canalith Jam
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sunkyunkwan University School of Medicine, Seoul, Korea. whchung@skku.edu
- 2Soree Ear Clinic, Seoul, Korea.
Abstract
- The authors report a 64-year-old man who developed persistent direction fixed nystagmus after a canalith repositioning maneuver for horizontal canal benign paroxysmal positional vertigo (HC-BPPV). The patient was initially diagnosed with right HC-BPPV given that the Dix-Hallpike test showed geotropic horizontal nystagmus that was more pronounced on the right side, although the roll test did not show any positional nystagmus. The patient was treated with a canalith repositioning maneuver (Lempert maneuver). The next day, the patient experienced a different character of dizziness, and left-beating spontaneous nystagmus regardless of head position was observed. After a forced prolonged left decubitus and frequent head shaking, his symptoms and nystagmus resolved. This condition, referred to as canalith jam, can be a complication after the repositioning maneuver in patients with BPPV. Atypical positional tests suggest that abnormal canal anatomy could be the underlying cause of canalith jam.
Figure
-
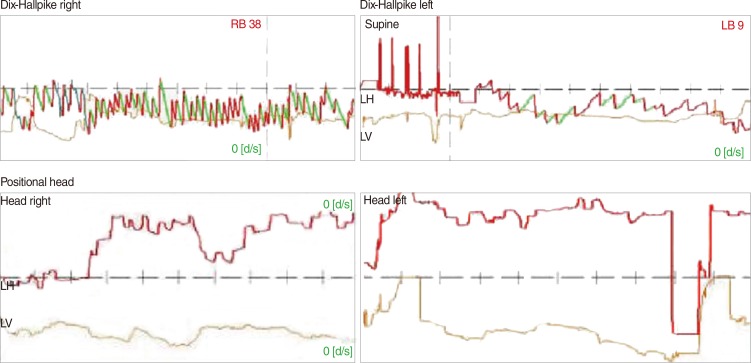
Fig. 1 Result of Dix-Hallpike test performed on initial visit. It showed bilateral horizontal geotropic nystagmus on the Dix-Hallpike test. The Dix-Hallpike test provoked horizontal nystagmus that was more pronounced on the right (38 deg/second) than on the left (9 deg/second). However, in positional roll test, there was no nystagmus recorded. RB, right beating; LB, left beating; LH, left horizontal; LV, left vertical.
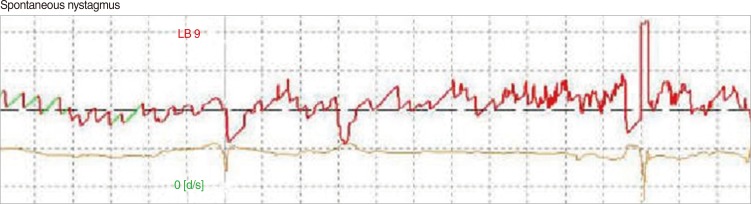
Fig. 2 Spontaneous nystagmus recorded on the day after the repositioning maneuver. It showed left-beating spontaneous nystagmus (9 deg/second). LB, left beating.

Fig. 3 Result of the Dix-Hallpike and positional test the day after the repositioning maneuver. It shows left-beating nystagmus independent of head position during the Dix-Hallpike test and positional test. The velocity of the nystagmus was greater after the Dix-Hallpike test than after the positional test. LB, left beating; LH, left horizontal; LV, left vertical; RH, right horizontal; RV, right vertical.
Reference
-
1. Lee SH, Kim JS. Benign paroxysmal positional vertigo. J Clin Neurol. 2010; 6. 6(2):51–63. PMID: 20607044.
Article2. Parnes LS, McClure JA. Free-floating endolymph particles: a new operative finding during posterior semicircular canal occlusion. Laryngoscope. 1992; 9. 102(9):988–992. PMID: 1518363.3. Epley JM. Human experience with canalith repositioning maneuvers. Ann N Y Acad Sci. 2001; 10. 942:179–191. PMID: 11710460.
Article4. Leigh RJ. Continuous vertigo and spontaneous nystagmus due to canalolithiasis of the horizontal canal. Neurology. 2001; 8. 57(4):745–746. PMID: 11524503.
Article5. Horii A, Kitahara T, Osaki Y, Imai T, Fukuda K, Sakagami M, et al. Intractable benign paroxysmal positioning vertigo: long-term follow-up and inner ear abnormality detected by three-dimensional magnetic resonance imaging. Otol Neurotol. 2010; 2. 31(2):250–255. PMID: 20042906.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Jamming of Horizontal Semicircular Canal Combined with Canalolithiasis of Contralateral Posterior Semicircular Canal
- Benign Paroxysmal Positional Vertigo
- Pathophysiology of Nystagmus in Benign Paroxysmal Positional Vertigo
- Outcome of canalith repositioning maneuver in Benign Paroxysmal Positional Vertigo
- Spontaneous Upbeat Nystagmus and Selective Anterior Semicircular Canal Hypofunction on Video Head Impulse Test: A New Variant of Canalith Jam?
