Chonnam Med J.
2009 Dec;45(3):182-187. 10.4068/cmj.2009.45.3.182.
Application of Image-Guided Radiation Therapy (IGRT) with Gold Markers in Prostate Cancer
- Affiliations
-
- 1Department of Urology, Hallym University Medical College, Seoul, Korea. uroyglee@hanafos.com
- 2Department of Radio-oncology, Hallym University Medical College, Seoul, Korea.
- KMID: 2274893
- DOI: http://doi.org/10.4068/cmj.2009.45.3.182
Abstract
- For image-guided radiation therapy (IGRT) of prostate cancer, gold markers called fiducials can be inserted into the prostate in advance. Here we examined the short-term results of IGRT for prostate cancer. We obtained the clinical data of 10 patients who underwent IGRT at the Department of Radiation Oncology in Kangnam Sacred Heart Hospital of Hallym University during March 2006 and July 2007. Three gold markers were implanted in the prostate before the radiotherapy. Exact focusing of the image was obtained by 3 gold markers on simple X-ray film or cone beam computed tomography during radiation therapy. The errors induced by setting up the patients during IGRT were examined. The setup errors, averaged over all patients, were -0.88 mm, 1.85 mm, and -0.40 mm in the left-right, cranial-caudal, and anterior-posterior directions, respectively. The motion of the prostate was greatest in the cranial-caudal (6.5 mm) direction. The post-radiation therapy prostate-specific antigen (PSA) level was decreased dramatically in all 10 patients. Two of three patients who had received hormonal therapy with IGRT showed a PSA nadir 12 months later without hormonal therapy. There were no peri-radiotherapy complications. Through the use of IGRT with gold markers, we could correct the setup errors that occur in conventional radiation therapy. Post-IGRT PSA was decreased dramatically. Even though our data are limited, we suggest that IGRT may be an effective radiation therapy modality for decreasing peri-radiotherapy complications and improving radiotherapy results in prostate cancer through exact focusing of the radiation.
Keyword
MeSH Terms
Figure
-
Fig. 1 Cliax iX with Cone-Beam CT.

Fig. 2 (A) Gold marker positions are Mkr1, Mkr2 and Mkr3 in the right base, left lateral and right apex of prostate. (B) Doctors may insert gold marker into the prostate by placing hollow gold needles through the rectum and moving a fiducial through each needle.

Fig. 3 Simple X-ray image showing three gold marker seeds.
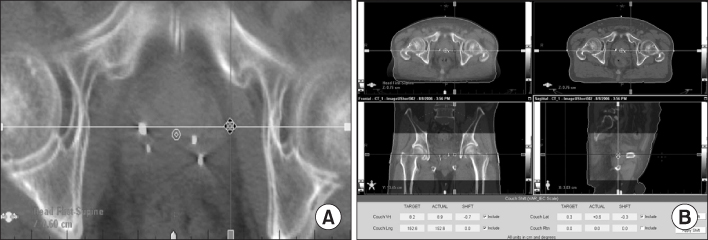
Fig. 4 (A) The CT image showing significant displacement of simulation CT and cone-beam CT images. (B) Fused image was corrected with displacement vector components.
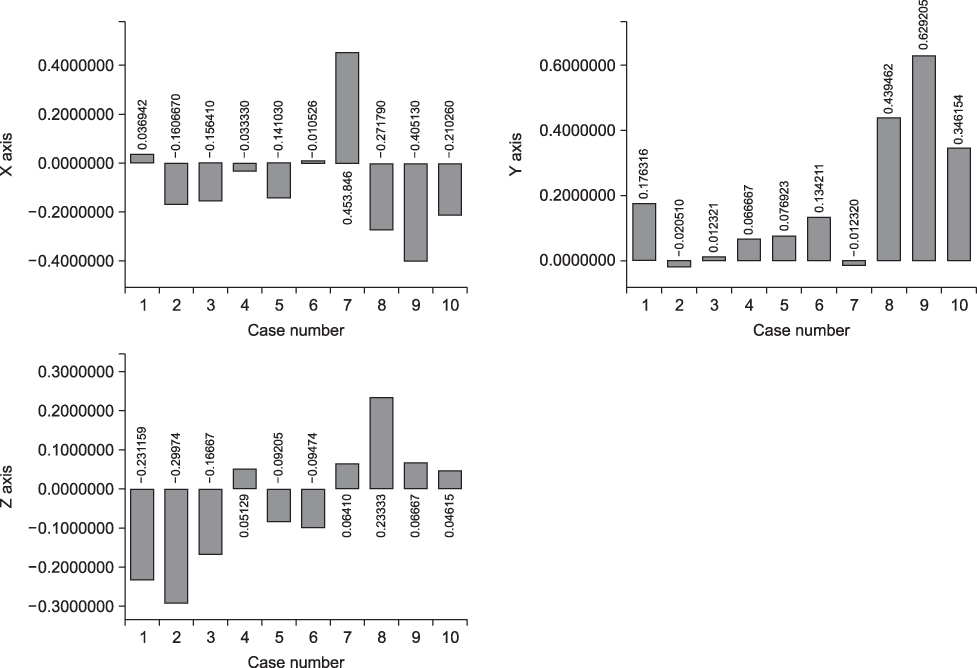
Fig. 5 Shifts along the principal directions of x-axis, y-axis and z-axis.
Reference
-
1. Bak JH, Jeong KK, Keum KC, Park SW. On-line image guided radiation therapy using cone-beam CT (CBCT). J Korean Soc Ther Radiol Oncol. 2006. 24:294–299.2. Burman C, Chui CS, Kutcher G, Leibel S, Zelefsky M, LoSasso T, et al. Planning, delivery, and quality assurance of intensity-modulated radiotherapy using dynamic multileaf collimator: a strategy for large-scale implementation for the treatment of carcinoma of the prostate. Int J Radiat Oncol Biol Phys. 1997. 39:863–873.
Article3. De Meerleer GO, Vakaet LA, De Gersem WR, De Wagter C, De Naeyer B, De Neve W. Radiotherapy of prostate cancer with or without intensity modulated beams: a planning comparison. Int J Radiat Oncol Biol Phys. 2000. 47:639–648.
Article4. Zelefsky MJ, Fuks Z, Happersett L, Lee HJ, Ling CC, Burman CM, et al. Clinical experience with intensity modulated radiation therapy (IMRT) in prostate cancer. Radiother Oncol. 2000. 55:241–249.
Article5. Nutting CM, Convey DY, Cosgrove VP, Rowbottom C, Padhani AR, Webb S, et al. Reduction of small and large bowel irradiation using an optimized intensity-modulated pelvic radiotherapy technique in patients with prostate cancer. Int J Radiat Oncol Biol Phys. 2000. 48:649–656.
Article6. Van Herk M. Errors and margins in radiotherapy. Semin Radiat Oncol. 2004. 14:52–64.
Article7. Hong JY, Rah JE, Suh TS. A study on image reconstruction for seed localization for permanent prostate brachytherapy. J Korean Soc Ther Radiol Oncol. 2007. 25:125–133.8. Langen KM, Zhang Y, Andrews RD, Hurley ME, Meeks SL, Poole DO, et al. Initial experience with megavoltage (MV) CT guidance for daily prostate alignments. Int J Radiat Oncol Biol Phys. 2005. 62:1517–1524.
Article9. Moseley DJ, White EA, Wiltshire KL, Rosewall T, Sharpe MB, Siewerdsen JN, et al. Comparison of localization performance with implanted fiducial markers and cone-beam computed tomography for on-line image-guided radiotherapy of the prostate. Int J Radiat Oncol Biol Phys. 2007. 67:942–953.
Article10. Hurkmans CW, Remeijer P, Lebesque JV, Mijnheer BJ. Set-up verification using portal imaging: review of current clinical practice. Radiother Oncol. 2001. 58:105–120.
Article11. Welsh JS, Berta C, Borzillary S, Sam C, Shickell D, Nobile L, et al. Fiducial markers implanted during prostate brachytherapy for guiding conformal external beam radiation therapy. Technol Cancer Res Treat. 2004. 3:359–364.
Article12. Henry AM, Stratford J, Davies J, McCarthy C, Swindell R, Sykes J, et al. An assessment of clinically optimal gold marker length and diameter for pelvic radiotherapy verification using an amorphous silicon flat panel electronic portal imaging device. Br J Radiol. 2005. 78:737–741.
Article13. Gladstone D, Hartford A, Marshall J. Gold coils used as fiducial markers of prostate location for image guided radiotherapy. 2005. In : Radiological Society of North America 2005 Annual Meeting; Chicago.14. Huisman H, Fütterer JJ, van Lin EN, Welmers A, Scheenen TW, van Dalen JA. Prostate cancer: precision of integrating functional MR imaging with radiation therapy treatment by using fiducial gold markers. Radiology. 2005. 236:311–317.
Article15. Shimizu S, Shirato H, Kitamura K, Shinohara N, Harabayashi T, Tsukamoto T, et al. Use of an implanted marker and real-time tracking of the marker for the positioning of prostate and bladder cancers. Int J Radiat Oncol Biol Phys. 2000. 48:1591–1597.
Article16. Hanks GE, Hanlon AI, Epsten B, Horwitz EM. Dose response in prostate cancer with 8-12 years' follow-up. Int J Radiat Oncol Biol Phys. 2002. 54:427–435.
Article17. Meyer JL, Leibel S, Roach M, Vijayakumar S. New technologies for the radiotherapy of prostate cancer. A discussion of clinical treatment programs. Front Radiat Ther Oncol. 2007. 40:315–337.18. Fisch BM, Pickett B, Weinberg V, Roach M. Dose of radiation received by the bulb of the penis correlates with risk of impotence after three-dimensional conformal radiotherapy for prostate cancer. Urology. 2001. 57:955–959.
Article19. Roach M, Winter K, Michalski JM, Cox JD, Purdy JA, Bosch W, et al. Penile bulb dose and impotence after three-dimensional conformal radiotherapy for prostate cancer on RTOG 9406: findings from a prospective, multi-institutional, phase I/II dose-escalation study. Int J Radiat Oncol Biol Phys. 2004. 60:1351–1356.
Article20. Kuban D, Pollack A, Huang E, Levy L, Dong L, Starkschall G, et al. Hazards of dose escalation in prostate cancer radiotherapy. Int J Radiat Oncol Biol Phys. 2003. 57:1260–1268.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Practical Considerations in Preparing an Institutional Procedure of Image Guided Radiation Therapy
- Image-guided radiation therapy in lymphoma management
- Interfraction Prostate Movement in Bone Alignment After Rectal Enema for Radiotherapy
- Strategic application of radiotherapy for hepatocellular carcinoma
- Application of surface-guided radiation therapy in prostate cancer: comparative analysis of differences with skin marking-guided patient setup
