Ann Rehabil Med.
2015 Feb;39(1):18-24. 10.5535/arm.2015.39.1.18.
Factors That Affect the Rehabilitation Duration in Patients With Congenital Muscular Torticollis
- Affiliations
-
- 1Department of Rehabilitation Medicine, Kwangju Christian Hospital, Gwangju, Korea. eykang74@hanmail.net
- KMID: 2273014
- DOI: http://doi.org/10.5535/arm.2015.39.1.18
Abstract
OBJECTIVE
To determine which factors affect the rehabilitation duration in patients with congenital muscular torticollis (CMT) and to predict the duration of rehabilitation and prognosis.
METHODS
One hundred and eighteen patients (79 males and 39 females) who were diagnosed with CMT and received physical therapy were enrolled in this study. We retrospectively reviewed the information in terms of sex, gestational age, birth weight, methods of delivery, fetal presentation, age at diagnosis, the affected sternocleidomastoid (SCM) muscle site, SCM muscle thickness, ratio of muscle thickness on the affected side to that on the unaffected side (called the 'abnormal/normal [A/N] ratio'), and range of motion for cervical rotation and side bending.
RESULTS
The SCM muscle thickness and A/N ratio had a positive linear relationship with the rehabilitation duration. Patients who were in the breech position needed longer rehabilitation. The birth weight and age at diagnosis were negatively correlated with the rehabilitation duration. However, the cervical range of motion, mass site, sex, gestational age, and methods of delivery were not correlated with the rehabilitation duration.
CONCLUSION
Patients with a thicker SCM, lower birth weight, and history of breech delivery had a longer rehabilitation duration.
Keyword
MeSH Terms
Figure
-
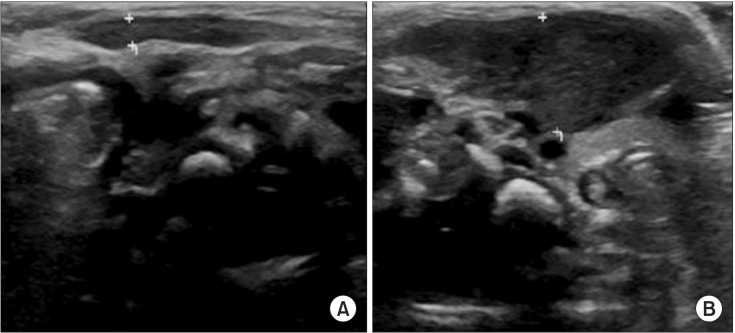
Fig. 1 Ultrasonographic findings of the sternocleidomastoid muscle in patients with congenital muscular torticollis. (A) Unaffected side and (B) affected side measurements at the thickest point in the longitudinal view.
Cited by 1 articles
-
Clinical Usefulness of Sonoelastography in Infants With Congenital Muscular Torticollis
Seong Kyung Hong, Jin Won Song, Seung Beom Woo, Jong Min Kim, Tae Eun Kim, Zee Ihn Lee
Ann Rehabil Med. 2016;40(1):28-33. doi: 10.5535/arm.2016.40.1.28.
Reference
-
1. Binder H, Eng GD, Gaiser JF, Koch B. Congenital muscular torticollis: results of conservative management with long-term follow-up in 85 cases. Arch Phys Med Rehabil. 1987; 68:222–225. PMID: 3566514.2. Cheng JC, Au AW. Infantile torticollis: a review of 624 cases. J Pediatr Orthop. 1994; 14:802–808. PMID: 7814599.3. Coventry MB, Harris LE. Congenital muscular torticollis in infancy; some observations regarding treatment. J Bone Joint Surg Am. 1959; 41A:815–822. PMID: 13664717.4. Suzuki S, Yamamuro T, Fujita A. The aetiological relationship between congenital torticollis and obstetrical paralysis. Int Orthop. 1984; 8:175–181. PMID: 6530313.
Article5. Yu CC, Wong FH, Lo LJ, Chen YR. Craniofacial deformity in patients with uncorrected congenital muscular torticollis: an assessment from three-dimensional computed tomography imaging. Plast Reconstr Surg. 2004; 113:24–33. PMID: 14707619.
Article6. Lee JY, Koh SE, Lee IS, Jung H, Lee J, Kang JI, et al. The cervical range of motion as a factor affecting outcome in patients with congenital muscular torticollis. Ann Rehabil Med. 2013; 37:183–190. PMID: 23705112.
Article7. Cheng JC, Tang SP, Chen TM. Sternocleidomastoid pseudotumor and congenital muscular torticollis in infants: a prospective study of 510 cases. J Pediatr. 1999; 134:712–716. PMID: 10356139.
Article8. Park JM, Choi JH, Lee YH. Ultrasonographic measurement of the sternocleidomastoid muscle in congenital muscular torticollis. J Korean Acad Rehabil Med. 1998; 22:955–959.9. Kim SY, Park MS, Yang JI, Yim SY. Comparison of helmet therapy and counter positioning for deformational plagiocephaly. Ann Rehabil Med. 2013; 37:785–795. PMID: 24466513.
Article10. Graf R. Classification of hip joint dysplasia by means of sonography. Arch Orthop Trauma Surg. 1984; 102:248–255. PMID: 6712426.
Article11. Kim MO, Kim SJ. Results of the conservative management of congenital muscular torticollis. J Korean Acad Rehabil Med. 1992; 16:42–50.12. Canale ST, Griffin DW, Hubbard CN. Congenital muscular torticollis: a long-term follow-up. J Bone Joint Surg Am. 1982; 64:810–816. PMID: 7085709.
Article13. Sanerkin NG, Edwards P. Birth injury to the sternomastoid muscle. J Bone Joint Surg Br. 1966; 48:441–447. PMID: 5950169.
Article14. Lee SJ, Han JD, Lee HB, Hwang JH, Kim SY, Park MC, et al. Comparison of clinical severity of congenital muscular torticollis based on the method of child birth. Ann Rehabil Med. 2011; 35:641–647. PMID: 22506186.
Article15. Emery C. The determinants of treatment duration for congenital muscular torticollis. Phys Ther. 1994; 74:921–929. PMID: 8090843.
Article16. Chang PY, Tan CK, Huang YF, Sheu JC, Wang NL, Yeh ML, et al. Torticollis: a long-term follow-up study. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi. 1996; 37:173–177. PMID: 8755170.17. Kim SJ, Park EM, Choi WK, Seo KS, Yoon JS, Lee EH. The Correlation between outcome and ultrasonographic findings in congenital muscular torticollis. J Korean Acad Rehabil Med. 2001; 25:601–608.18. Lee YT, Jahng JS, Park BM. A clinical study of congenital muscular torticollis. J Korean Orthop Assoc. 1986; 21:423–432.
Article19. Han JD, Kim SH, Lee SJ, Park MC, Yim SY. The thickness of the sternocleidomastoid muscle as a prognostic factor for congenital muscular torticollis. Ann Rehabil Med. 2011; 35:361–368. PMID: 22506145.
Article20. Han SJ, Shin BM, Lee JM, Yoon TS. Factors affecting rehabilitation outcome of congenital muscular torticollis. J Korean Acad Rehabil Med. 2010; 34:643–649.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Familial Congenital Muscular Torticollis: A Case Report
- Two Cases of Sternomastoid Tumor
- Congenital Torticollis with Bilateral Sternocleidomastoid Muscle Contracture
- Congenital Muscular Torticollis in Siblings: A case report and literature review
- Ultrasonographic Measurement of the Sternocleidomastoid Muscle in Congenital Muscular Torticollis
