Usefulness of Ultrasonography to Predict Response to Injection Therapy in Carpal Tunnel Syndrome
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Korea University College of Medicine, Seoul 152-703, Korea. rehab46@korea.ac.kr
- KMID: 2266859
- DOI: http://doi.org/10.5535/arm.2011.35.3.388
Abstract
OBJECTIVE
To verify the feasibility of initial parameters of ultrasonography or electromyography for the prediction of effect after steroid injection therapy in a carpal tunnel syndrome (CTS) patient. METHOD: We recruited individuals with clinical and electrodiagnostic evidence of CTS. Results from the Boston self-assessment questionnaire, median motor and sensory nerve conduction studies, and median nerve ultrasonography were evaluated at baseline, 1 month, and 6 months after injection. Evaluation of median nerve ultrasonography parameters included measurements taken at the maximal swelling point (MS), 2 cm proximal from MS (2MS), and 12 cm proximal from MS (12MS), and its ratio (MS/12MS, 2MS/12MS) was calculated. The correlation between improvement of the symptom score after treatment and baseline parameters was estimated.
RESULTS
Fourteen individuals (14 women, mean age 53.8 years) with 22 affected wrists were enrolled. After steroid injection therapy, clinical and electromyographic parameters showed significant improvements at 1 month or 6 months after injection, and ultrasonographic parameters showed significant changes in maximal area and area ratio (MS/12MS) of the median nerve. Symptom score improvement showed a positive correlation in the initial 2MS and ratio of 2MS/12MS after 6 months (p<0.05).
CONCLUSION
Most of the improvements occurred during the first month after injection and lasted up to 6 months. The initial median nerve swelling and its ratio may be a useful predictor of response after steroid injection.
MeSH Terms
Figure
-
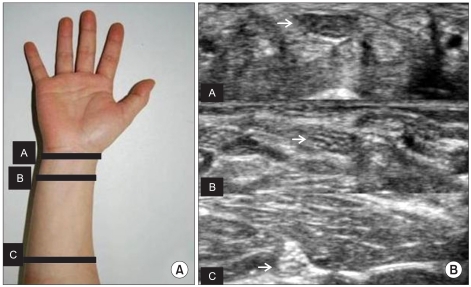
Fig. 1 (A) Placement of ultrasonographic probe at the forearm. Ultrasonographic transverse scan was done at 3 different levels. We measured the cross sectional area of median nerve at the most swollen site level A, 2 cm proximal to this level B, 12 cm proximal to this level C. We calculated ratio of A/C, B/C. (B) Median nerve transverse sonogram image at A, B, C level.
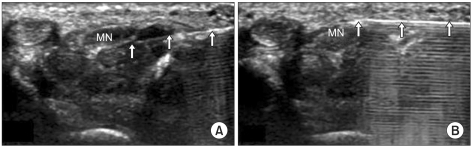
Fig. 2 Transverse sonogram of the carpal tunnel in a patient with idiopathic carpal tunnel syndrome. (A) A 26-gauge needle (arrow) is shown passing from the ulnar aspect of the carpal tunnel to a position adjacent and deep to the median nerve. (B) A 26-gauge needle (arrow) is shown passing from the ulnar aspect of the carpal tunnel to a position adjacent to the median nerve just below flexor retinaculum. MN: Median nerve .
Cited by 1 articles
-
Carpal Tunnel Syndrome Assessment With Ultrasonography: A Comparison Between Non-diabetic and Diabetic Patients
Chung Ho Lee, Hanboram Choi, Joon Shik Yoon, Seok Kang
Ann Rehabil Med. 2018;42(1):85-91. doi: 10.5535/arm.2018.42.1.85.
Reference
-
1. Gelberman RH, Rydevik BL, Pess GM, Szabo RM, Lundborg G. Carpal tunnel syndrome. A scientific basis for clinical care. Orthop Clin North Am. 1988; 19:115–124. PMID: 3275920.2. Lee D, van Holsbeeck MT, Janevski PK, Ganos DL, Ditmars DM, Darian VB. Diagnosis of carpal tunnel syndrome. Ultrasound versus electromyography. Radiol Clin North Am. 1999; 37:859–872. PMID: 10442084.3. Jablecki CK, Andary MT, Floeter MK, Miller RG, Quartly CA, Vennix MJ, Wilson JR. Practice parameter: Electrodiagnostic studies in carpal tunnel syndrome. Report of the American Association of Electrodiagnostic Medicine, American Academy of Neurology, and the American Academy of Physical Medicine and Rehabilitation. Neurology. 2002; 58:1589–1592. PMID: 12058083.
Article4. Wong SM, Griffith JF, Hui AC, Lo SK, Fu M, Wong KS. Carpal tunnel syndrome: diagnostic usefulness of sonography. Radiology. 2004; 232:93–99. PMID: 15155897.
Article5. Racasan O, Dubert T. The safest location for steroid injection in the treatment of carpal tunnel syndrome. J Hand Surg Br. 2005; 30:412–414. PMID: 15950338.
Article6. Lee JH, An JH, Lee SH, Hwang EY. Effectiveness of steroid injection in treating patients with moderate and severe degree of carpal tunnel syndrome measured by clinical and electrodiagnostic assessment. Clin J Pain. 2009; 25:111–115. PMID: 19333155.
Article7. Milo R, Kalichman L, Volchek L, Reitblat T. Local corticosteroid treatment for carpal tunnel syndrome: a 6-month clinical and electrophysiological follow-up study. J Back Musculoskelet Rehabil. 2009; 22:59–64. PMID: 20023332.
Article8. Ucan H, Yagci I, Yilmaz L, Yagmurlu F, Keskin D, Bodur H. Comparison of splinting, splinting plus local steroid injection and open carpal tunnel release outcomes in idiopathic carpal tunnel syndrome. Rheumatol Int. 2006; 27:45–51. PMID: 16871409.
Article9. Cho JM, Yoon JS, Kim SJ, Park BK, Lee GH, Jeong JS. Feasibility of ultrasonographic area ratio of median nerve in the diagnosis of carpal tunnel syndrome in Korea. J Korean Acad Rehabil Med. 2009; 33:627–631.10. Smith J, Wisniewski SJ, Finnoff JT, Payne JM. Sonographically guided carpal tunnel injections: the ulnar approach. J Ultrasound Med. 2008; 27:1485–1490. PMID: 18809959.11. Armstrong T, Devor W, Borschel L, Contreras R. Intracarpal steroid injection is safe and effective for short-term management of carpal tunnel syndrome. Muscle Nerve. 2004; 29:82–88. PMID: 14694502.
Article12. Hui AC, Wong S, Leung CH, Tong P, Mok V, Poon D, Li-Tsang CW, Wong LK, Boet R. A randomized controlled trial of surgery vs steroid injection for carpal tunnel syndrome. Neurology. 2005; 64:2074–2078. PMID: 15985575.
Article13. Hagebeuk EE, de Weerd AW. Clinical and electrophysiological follow-up after local steroid in jec tion in the carpal tunnel syndrome. Clin Neurophysiol. 2004; 115:1464–1468. PMID: 15134716.14. Mondelli M, Filippou G, Aretini A, Frediani B, Reale F. Ultrasonography before and after surgery in carpal tunnel syndrome and relationship with clinical and electrophysiological findings. A new outcome predictor? Scand J Rheumatol. 2008; 37:219–224. PMID: 18465458.
Article15. Naranjo A, Ojeda S, Arana V, Baeta P, Fernandez-Palacios J, Garcia-Duque O, Rodriguez-Lozano C, Carmona L. Usefulness of clinical findings, nerve conduction studies and ultrasonography to predict response to surgical release in idiopathic carpal tunnel syndrome. Clin Exp Rheumatol. 2009; 27:786–793. PMID: 19917161.16. Abicalaf CA, de Barros N, Sernik RA, Pimentel BF, Braga-Baiak A, Braga L, Houvet P, Brasseur JL, Roger B, Cerri GG. Ultrasound evaluation of patients with carpal tunnel syndrome before and after endoscopic release of the transverse carpal ligament. Clin Radiol. 2007; 62:891–894. PMID: 17662738.
Article17. Colak A, Kutlay M, Pekkafali Z, Saracoglu M, Demircan N, Simsek H, Akin ON, Kibici K. Use of sonography in carpal tunnel syndrome surgery. A prospective study. Neurol Med Chir. 2007; 47:109–115.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Usefulness of Ultrasound for Carpal Tunnel Syndrome Proven in Meta-Analysis Studies
- Ultrasound-Guided Nerve Hydrodissection for Carpal Tunnel Syndrome
- The Abnormal Ultrasonographic Findings of Carpal Tunnel in Carpal Tunnel Syndrome
- Extraskeletal Chondroma Causing Carpal Tunnel Syndrome: A Case Report
- RE: Value of Power Doppler and Gray-Scale US in the Diagnosis of Carpal Tunnel Syndrome: Contribution of Cross-Sectional Area just before the Tunnel Inlet as Compared with the Cross-Sectional Area at the Tunnel
