Cauda Equina Syndrome Caused by Spinal Dural Arteriovenous Fistula
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan 602-739, Korea. wanykim920@gmail.com
- 2Department of Radiology, Pusan National University School of Medicine, Busan 602-739, Korea.
- KMID: 2266820
- DOI: http://doi.org/10.5535/arm.2011.35.6.928
Abstract
- Spinal dural arteriovenous fistula (SDAVF) is rare but still the most commonly encountered vascular malformation of the spinal cord. A 31-year-old male developed gait disturbance due to weakness of his lower extremities, voiding difficulty and sexual dysfunction with a progressive course since 3 months. He showed areflexia in both knees and ankles. Electromyographic findings were suggestive of multiple root lesions involving bilateral L2 to S4 roots of moderate degree. Magnetic resonance images showed high signal intensity with an ill-defined margin in T2-weighted images and intensely enhanced by a contrast agent through the lumbosacral spinal cord. Selective spinal angiography confirmed a dural arteriovenous fistula with a nidus at the L2 vertebral level. After selective endovascular embolization, his symptoms drastically improved except sexual dysfunction. We report a rare case of cauda equina syndrome due to spinal arteriovenous fistula with drastic improvement after endovascular embolization.
MeSH Terms
Figure
-
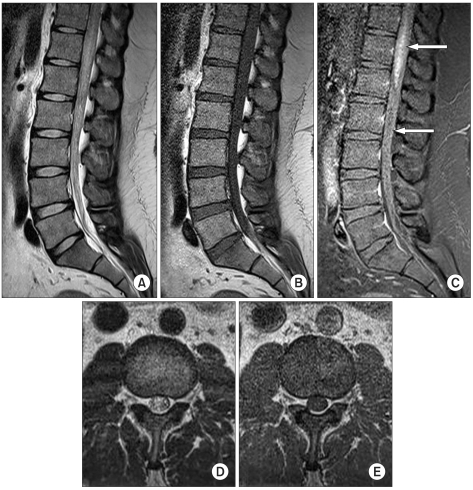
Fig. 1 T2-weighted magnetic resonance (MR) images (A, D) show central intramedullary hyperintensity of the distal cord and cauda equina as a sign of central myelopathy with extensive spinal cord edema. T1-weighted (B, E), pregadolinium and (C) postgadolinium MR images demonstrate intramedullary hyperintensity with flow voids (white arrow) on the dorsal aspect of the spinal cord corresponding to the dilated perimedullary veins.
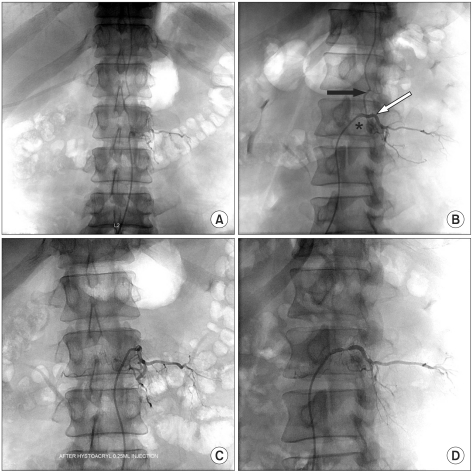
Fig. 2 Spine anteroposterior angiogram with selective catheterization of the left L2 segmental artery (white arrow) shows a fistula draining to the perimedullary vein (black arrow) (A, B). A small sac (asterisk) is noted near the fistula which is not observed in typical dural arteriovenous fistulas (B). After embolization using a NBCA/lipiodol mixture, no further residual perfusion of the fistula was demonstrated (C, D).
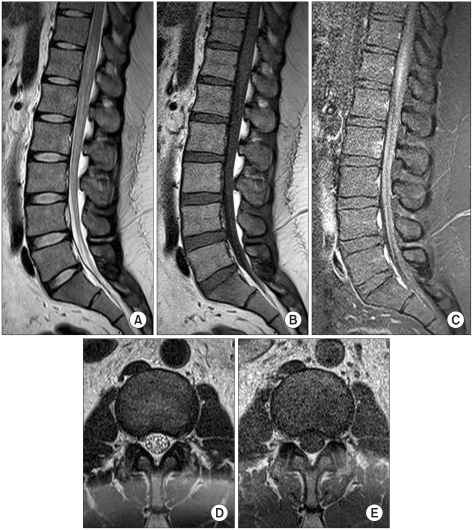
Fig. 3 T2-weighted (A, D), T1-weighted (B, E), pregadolinium and (C) postgadolinium spinal MR images performed 2 weeks after endovascular embolization. Compared to previous MR images (Fig. 1), they show reduced enhancement and edema of the distal cord with diminished flow voids.
Reference
-
1. Kendall BE, Logue V. Spinal epidural angiomatous malformations draining into intrathecal veins. Neuroradiology. 1977; 13:181–189. PMID: 876450.
Article2. Krings T, Geibprasert S. Spinal dural arteriovenous fistulas. Am J Neuroradiol. 2009; 30:639–648. PMID: 19213818.
Article3. Jellema K, Canta LR, Tijssen CC, van Rooij WJ, Koudstaal PJ, van Gijn J. Spinal dural arteriovenous fistulas: clinical features in 80 patients. J Neurol Neurosurg Psychiatry. 2003; 74:1438–1440. PMID: 14570843.
Article4. Koch C. Spinal dural arteriovenous fistula. Curr Opin Neurol. 2006; 19:69–75. PMID: 16415680.
Article5. Foix C, Alajouanine T. Subacute necrotic myelitis, slowly progressive central myelitis with vacular hyper plasia, and slowly ascending, increasingly flaccid amyotrophic paraplegia accompanied by albuminocytologic dissociation. Rev Neurol. 1926; 33:1–42.6. Schick U, Hassler W. Treatment and outcome of spinal dural arteriovenous fistulas. Eur Spine J. 2003; 12:350–355. PMID: 12955607.
Article7. Park SB, Han MH, Jahng TA, Kwon BJ, Chung CK. Spinal dural arteriovenous fistulas: clinical experience with endovascular treatment as a primary therapeutic modality. J Korean Neurosurg Soc. 2008; 44:364–369. PMID: 19137080.
Article8. Prieto R, Pascual JM, Gutierrez R, Santos E. Recovery from paraplegia after the treatment of spinal dural arteriovenous fistula: case report and review of the literature. Acta Neurochir (Wien). 2009; 151:1385–1397. PMID: 19618103.
Article9. Hassler W, Thorn A, Grote EH. Hemodynamics of spinal dural arteriovenous fistulas. An intraoperative study. J Neurosurg. 1989; 70:360–370. PMID: 2492595.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cauda Equina Syndrome after Spinal Manipulative Therapy: A case report
- Cavernous Hemangioma of the Cauda Equina
- Endovascular Treatment of Spinal Dural and Epidural Arteriovenous Fistula as Complication of Lumbar Surgery
- Cauda Equina Syndrome Occurred by Adhesive Arachnoiditis of the Lumbar Spine with an Unknown Cause
- Lumbar Spinal Epidural Abscess Combined with Cauda Equina Syndrome: A Case Report
