Ann Rehabil Med.
2013 Aug;37(4):516-522. 10.5535/arm.2013.37.4.516.
Effects on Foot External Rotation of the Modified Ankle-Foot Orthosis on Post-Stroke Hemiparetic Gait
- Affiliations
-
- 1Department of Rehabilitation Medicine, Sangju Seongmo Hospital, Sangju, Korea.
- 2Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. mhchun@amc.seoul.kr
- 3Department of Rehabilitation Medicine, Jeju National University Hospital, Jeju, Korea.
- KMID: 2266607
- DOI: http://doi.org/10.5535/arm.2013.37.4.516
Abstract
OBJECTIVE
To evaluate the effects of heel-opened ankle foot orthosis (HOAFO) on hemiparetic gait after stroke, especially on external foot rotation, and to compare the effects of HOAFO with conventional plastic-AFO (pAFO) and barefoot during gait.
METHODS
This cross-over observational study involved 15 hemiparetic patients with external rotation of the affected foot. All subjects were able to walk independently, regardless of their usual use of a single cane, and had a less than fair-grade in ankle dorsiflexion power. Each patient was asked to walk in three conditions with randomized sequences: 1) barefoot, 2) with a pAFO, and 3) with an HOAFO. Their gait patterns were analyzed using a motion analysis system.
RESULTS
Fifteen patients consisted of nine males and six females. On gait analysis, hip and foot external rotation were significantly greater in pAFO (-3.35degrees and -23.68degrees) than in barefoot and HOAFO conditions (p<0.05). Wearing an HOAFO resulted in significant decreases in hip (0.78degrees, p=0.04) and foot (-17.99degrees, p<0.01) external rotation compared with pAFO; although there was no significant difference between HOAFO and barefoot walking. Walking speed and percentage of single limb support were significantly greater for HOAFO than in barefoot walking.
CONCLUSION
HOAFO was superior to pAFO in reducing hip and foot external rotation during the stance phase in patients with post-stroke hemiparesis. HOAFO may, therefore, be useful in patients with excessive external rotation of the foot during conventional pAFO.
Keyword
MeSH Terms
Figure
-
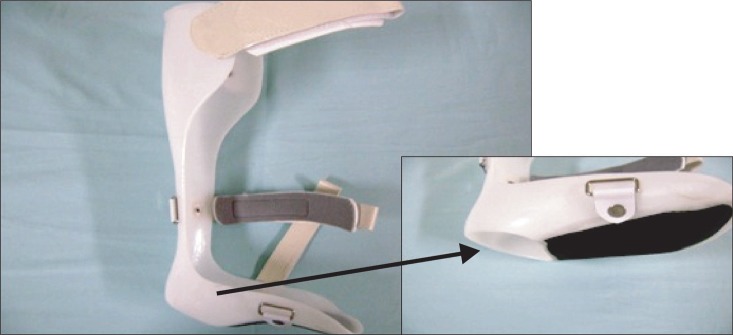
Fig. 1 Left heel-opened ankle foot orthosis. Heel of plastic ankle-foot orthosis was cut to reduce external rotation of foot during stance phase.
Reference
-
1. da Cunha-Filho IT, Henson H, Wankadia S, Protas EJ. Reliability of measures of gait performance and oxygen consumption with stroke survivors. J Rehabil Res Dev. 2003; 40:19–25. PMID: 15150717.2. Olney SJ, Monga TN, Costigan PA. Mechanical energy of walking of stroke patients. Arch Phys Med Rehabil. 1986; 67:92–98. PMID: 3954572.
Article3. Kim CM, Eng JJ. Magnitude and pattern of 3D kinematic and kinetic gait profiles in persons with stroke: relationship to walking speed. Gait Posture. 2004; 20:140–146. PMID: 15336283.
Article4. Cruz TH, Dhaher YY. Impact of ankle-foot-orthosis on frontal plane behaviors post-stroke. Gait Posture. 2009; 30:312–316. PMID: 19570678.
Article5. de Wit DC, Buurke JH, Nijlant JM, Ijzerman MJ, Hermens HJ. The effect of an ankle-foot orthosis on walking ability in chronic stroke patients: a randomized controlled trial. Clin Rehabil. 2004; 18:550–557. PMID: 15293489.
Article6. Embrey DG, Holtz SL, Alon G, Brandsma BA, McCoy SW. Functional electrical stimulation to dorsiflexors and plantar flexors during gait to improve walking in adults with chronic hemiplegia. Arch Phys Med Rehabil. 2010; 91:687–696. PMID: 20434604.
Article7. Sheffler LR, Hennessey MT, Naples GG, Chae J. Peroneal nerve stimulation versus an ankle foot orthosis for correction of footdrop in stroke: impact on functional ambulation. Neurorehabil Neural Repair. 2006; 20:355–360. PMID: 16885421.
Article8. Cakar E, Durmus O, Tekin L, Dincer U, Kiralp MZ. The ankle-foot orthosis improves balance and reduces fall risk of chronic spastic hemiparetic patients. Eur J Phys Rehabil Med. 2010; 46:363–368. PMID: 20927002.9. Gok H, Kucukdeveci A, Altinkaynak H, Yavuzer G, Ergin S. Effects of ankle-foot orthoses on hemiparetic gait. Clin Rehabil. 2003; 17:137–139. PMID: 12625653.
Article10. Chen CC, Hong WH, Wang CM, Chen CK, Wu KP, Kang CF, et al. Kinematic features of rear-foot motion using anterior and posterior ankle-foot orthoses in stroke patients with hemiplegic gait. Arch Phys Med Rehabil. 2010; 91:1862–1868. PMID: 21112427.
Article11. Roth EJ, Merbitz C, Mroczek K, Dugan SA, Suh WW. Hemiplegic gait: relationships between walking speed and other temporal parameters. Am J Phys Med Rehabil. 1997; 76:128–133. PMID: 9129519.12. Joo BG, Yoo JY, Ha SB. Effect of torque heel on excessive external rotation of hemiplegic foot : three dimensional gait analysis. J Korean Acad Rehabil Med. 1998; 22:1114–1122.13. Lee JK, Lim OK, Yim YM, Chung SR, Bae KH, Kim SH, et al. The shoes designed to inhibit excessive external rotation of hemiplegic foot with plastic ankle foot orthosis: a case report. J Korean Acad Rehabil Med. 2006; 30:94–97.14. Bohannon RW, Smith MB. Interrater reliability of a Modified Ashworth Scale of muscle spasticity. Phys Ther. 1987; 67:206–207. PMID: 3809245.
Article15. Miyamoto S, Kondo T, Suzukamo Y, Michimata A, Izumi S. Reliability and validity of the Manual Function Test in patients with stroke. Am J Phys Med Rehabil. 2009; 88:247–255. PMID: 19106794.
Article16. Cameron D, Bohannon RW. Criterion validity of lower extremity Motricity Index scores. Clin Rehabil. 2000; 14:208–211. PMID: 10763800.
Article17. Blum L, Korner-Bitensky N. Usefulness of the Berg Balance Scale in stroke rehabilitation: a systematic review. Phys Ther. 2008; 88:559–566. PMID: 18292215.
Article18. Levens AS, Inman VT, Blosser JA. Transverse rotation of the segments of the lower extremity in locomotion. J Bone Joint Surg Am. 1948; 30A:859–872. PMID: 18887290.
Article19. Johnston RC, Smidt GL. Measurement of hip-joint motion during walking: evaluation of an electrogoniometric method. J Bone Joint Surg Am. 1969; 51:1082–1094. PMID: 5805410.20. Lyons K, Perry J, Gronley JK, Barnes L, Antonelli D. Timing and relative intensity of hip extensor and abductor muscle action during level and stair ambulation: an EMG study. Phys Ther. 1983; 63:1597–1605. PMID: 6622534.21. Saunders JB, Inman VT, Eberhart HD. The major determinants in normal and pathological gait. J Bone Joint Surg Am. 1953; 35-A:543–558. PMID: 13069544.
Article22. Murray MP. Gait as a total pattern of movement. Am J Phys Med. 1967; 46:290–333. PMID: 5336886.23. Wagenaar RC, Beek WJ. Hemiplegic gait: a kinematic analysis using walking speed as a basis. J Biomech. 1992; 25:1007–1015. PMID: 1517261.
Article24. De Quervain IA, Simon SR, Leurgans S, Pease WS, McAllister D. Gait pattern in the early recovery period after stroke. J Bone Joint Surg Am. 1996; 78:1506–1514. PMID: 8876578.25. Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Recovery of walking function in stroke patients: the Copenhagen Stroke Study. Arch Phys Med Rehabil. 1995; 76:27–32. PMID: 7811170.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of Torque Heel on Excessive External Rotation of Hemiplegic Foot: Three Dimensional Gait Analysis
- Effects of Ankle Foot Orthosis on Post-stroke Hemiplegic Gait -A Meta-analysis-
- The Shoes Designed to Inhibit Excessive External Rotation of Hemiplegic Foot with Plastic Ankle Foot Orthosis: A case report
- Effect of Plastic Ankle Foot Orthosis and Functional Electrical Stimulation on Hemiplegic Gait
- Effects of Plastic Ankle-Foot Orhtosis on Hemiplegic Ambulation
