Diagnosis With Manometry and Treatment With Repetitive Transcranial Magnetic Stimulation in Dysphagia
- Affiliations
-
- 1Department of Rehabilitation Medicine, Yeouido St. Mary's Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea. sae_byuk@hotmail.com
- KMID: 2266573
- DOI: http://doi.org/10.5535/arm.2013.37.6.907
Abstract
- Videofluoroscopic swallowing study (VFSS) used for the diagnosis of dysphagia has limitations in objectively assessing the contractility of the pharyngeal muscle or the degree of the upper esophageal sphincter relaxation. With a manometer, however, it is possible to objectively assess the pressure changes in the pharynx caused by pharyngeal muscle contraction during swallowing or upper esophageal sphincter relaxation, hence remedying the limitations of VFSS. The following case report describes a patient diagnosed with lateral medullar infarction presenting a 52-year-old male who had dysphagia. We suggested that the manometer could be used to assess the specific site of dysfunction in patients with dysphagia complementing the limitations of VFSS. We also found that repetitive transcranial magnetic stimulation was effective in treating patients refractory to traditional dysphagia rehabilitation.
MeSH Terms
Figure
-
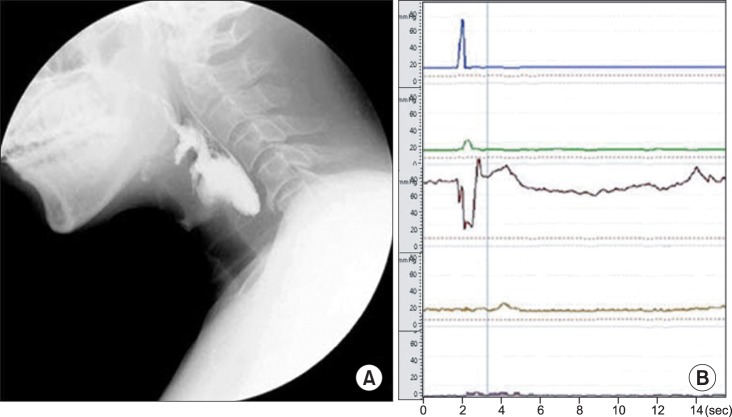
Fig. 1 Videofluoroscopic swallowing study finding (A) and manometry finding (B) before repetitive transcranial magnetic stimulation. The pressure changes in the pharynx and oesophagus were recorded using a 5-lumen perfused catheter system. The plots are: 10 cm upper of the UES (blue line), 5 cm upper of the UES (green line), UES (brown line), 5 cm lower of the UES (yellow line), 10 cm lower of the UES (purple line). The pressure increase was reduced at the site 5 cm upper of the UES (green line). The decreased pressure due to UES relaxation was clear (brown line), but the retained foods not passing by the UES due to the reduced duration was observed. In addition, no pressure change caused by peristalsis was observed due to the retained foods did not pass by the esophageal body. UES, upper esophageal sphincter.
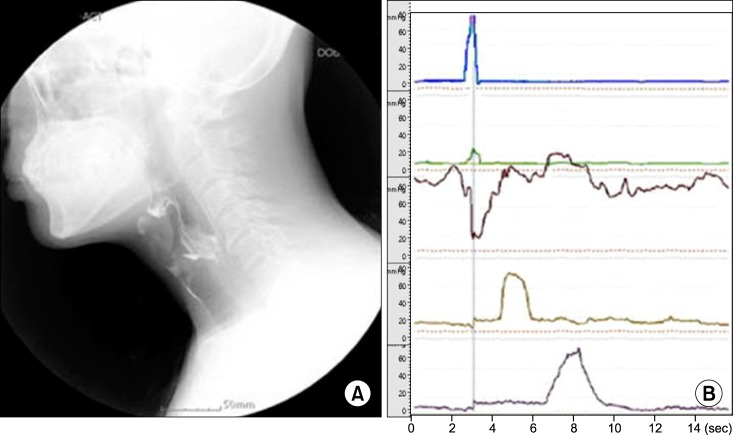
Fig. 2 Videofluoroscopic swallowing study finding (A) and manometry finding (B) after the 2-week repetitive transcranial magnetic stimulation treatment. Compared to the status observed 2 weeks prior, no significant increase in the pressure change at the site 5 cm upper of the UES was observed. However, foods passed by the UES due to the extended duration of UES relaxation, and peristalsis were also observed in the esophageal body. UES, upper esophageal sphincter.
Reference
-
1. Singh S, Hamdy S. Dysphagia in stroke patients. Postgrad Med J. 2006; 82:383–391. PMID: 16754707.
Article2. Sessle BJ, Henry JL. Neural mechanisms of swallowing: neurophysiological and neurochemical studies on brain stem neurons in the solitary tract region. Dysphagia. 1989; 4:61–75. PMID: 2484181.
Article3. Higo R, Tayama N, Watanabe T. Manometric abnormality in dysphagic patients after medullary cerebrovascular accidents. ORL J Otorhinolaryngol Relat Spec. 2002; 64:368–372. PMID: 12417783.
Article4. Jean A. Brainstem organization of the swallowing network. Brain Behav Evol. 1984; 25:109–116. PMID: 6100081.
Article5. Hila A, Castell JA, Castell DO. Pharyngeal and upper esophageal sphincter manometry in the evaluation of dysphagia. J Clin Gastroenterol. 2001; 33:355–361. PMID: 11606849.
Article6. Khedr EM, Abo-Elfetoh N. Therapeutic role of rTMS on recovery of dysphagia in patients with lateral medullary syndrome and brainstem infarction. J Neurol Neurosurg Psychiatry. 2010; 81:495–499. PMID: 19828479.
Article7. Jefferson S, Mistry S, Michou E, Singh S, Rothwell JC, Hamdy S. Reversal of a virtual lesion in human pharyngeal motor cortex by high frequency contralesional brain stimulation. Gastroenterology. 2009; 137:841–849. PMID: 19427312.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Application of Non-invasive Brain Stimulation on Dysphagia after Stroke
- Predictors of Response to Repetitive Transcranial Magnetic Stimulation in Depression: A Review of Recent Updates
- Repetitive Transcranial Magnetic Stimulation for Limb-Kinetic Apraxia in Parkinson's Disease
- Treatment-Resistant Depression Entering Remission Following a Seizure during the Course of Repetitive Transcranial Magnetic Stimulation
- Early Augmentation Response with Low-frequency Repetitive Transcranial Magnetic Stimulation in Treatment Resistant Depression
