Ann Dermatol.
2009 Aug;21(3):221-225. 10.5021/ad.2009.21.3.221.
Surgery and Perioperative Intralesional Corticosteroid Injection for Treating Earlobe Keloids: A Korean Experience
- Affiliations
-
- 1Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, Korea. kychung@yuhs.ac
- KMID: 2266280
- DOI: http://doi.org/10.5021/ad.2009.21.3.221
Abstract
-
BACKGROUND: The aesthetic implications of ear keloids, which affect people of all races, are serious and the treatment of earlobe keloids is known to be difficult. The high rate of recurrence following excision alone has led to investigating various types of adjuvant therapy, including intralesional corticosteroid injection.
OBJECTIVE
We evaluated the efficacy of excision combined with perioperative intralesional triamcinolone acetonide injection for treating earlobe keloids of Korean patients.
METHODS
From 1997 to 2006, eighteen keloids on the earlobes of fifteen Korean patients were treated. The patient age ranged from 15 to 32 years (mean age: 24 years). All the patients were female and the keloids occurred after ear piercing. Preoperative intralesional triamcinolone acetonide (TA) injection was administered twice at a 1-month interval. Postoperative intralesional TA injections were given every 1 month for several months, depending on the patient's clinical progress.
RESULTS
The follow-up period ranged from 4 to 42 months (mean: 18.5 months). After the surgery, TA intralesional injections were given 2 to 13 times (mean: 5.2 times). Of the treated keloids, eleven showed good results (61.1%) and three recurred (16.6%). No complications from the TA intralesional injection were observed.
CONCLUSION
Among the various treatments for earlobe keloids, we suggest that excision with corticosteroid intralesional injection can be used as the first line therapy when considering its effect and economic advantage.
MeSH Terms
Figure
-
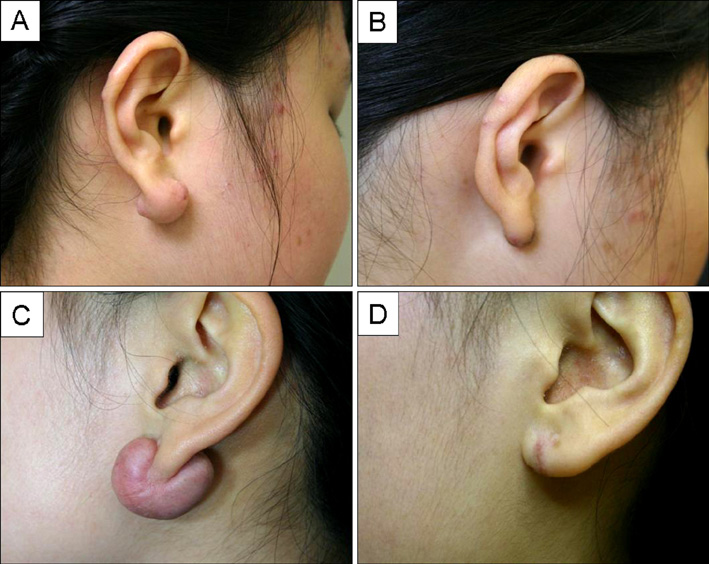
Fig. 1 (A) Patient 4's earlobe keloid before treatment and (B) 6 months after surgery. (C) Patient 11's earlobe keloid before treatment and (D) 3 months after surgery.
Cited by 1 articles
-
Postoperative Electron Beam Radiotherapy for Keloids: Treatment Outcome and Factors Associated with Occurrence and Recurrence
Sun Young Lee, Jin Park
Ann Dermatol. 2015;27(1):53-58. doi: 10.5021/ad.2015.27.1.53.
Reference
-
1. Kelly AP. Parish LC, Lask GP, editors. Keloids and hypertrophic scars. Aesthetic dermatology. 1991. New York: McGraw-Hill;58–64.2. Cheng LH. Keloid of the ear lobe. Laryngoscope. 1972. 82:673–681.
Article3. Stucker FJ, Shaw GY. An approach to management of keloids. Arch Otolaryngol Head Neck Surg. 1992. 118:63–67.
Article4. Cosman B, Crikelair GF, Ju DM. The surgical treatment of keloids. Plast Reconstr Surg. 1961. 27:335–345.
Article5. Oluwasanmi JO. Keloids in the African. Clin Plast Surg. 1974. 1:179–195.
Article6. Alhady SM, Sivanantharajah K. Keloids in various races. A review of 175 cases. Plast Reconstr Surg. 1969. 44:564–566.
Article7. Arnold HL Jr, Grauer FH. Keloids: etiology, and management by excision and intensive prophylactic radiation. Arch Dermatol. 1959. 80:772–777.
Article8. Shons AR, Press BH. The treatment of earlobe keloids by surgical excision and postoperative triamcinolone injection. Ann Plast Surg. 1983. 10:480–482.
Article9. Sallstrom KO, Larson O, Heden P, Eriksson G, Glas JE, Ringborg U. Treatment of keloids with surgical excision and postoperative X-ray radiation. Scand J Plast Reconstr Surg Hand Surg. 1989. 23:211–215.
Article10. Mercer DM, Studd DM. "Oyster splints": a new compression device for the treatment of keloid scars of the ear. Br J Plast Surg. 1983. 36:75–78.
Article11. Fulton JE Jr. Silicone gel sheeting for the prevention and management of evolving hypertrophic and keloid scars. Dermatol Surg. 1995. 21:947–951.
Article12. Rusciani L, Rossi G, Bono R. Use of cryotherapy in the treatment of keloids. J Dermatol Surg Oncol. 1993. 19:529–534.
Article13. Berman B, Flores F. Recurrence rates of excised keloids treated with postoperative triamcinolone acetonide injections or interferon alfa-2b injections. J Am Acad Dermatol. 1997. 37:755–757.
Article14. Lee Y, Minn KW, Baek RM, Hong JJ. A new surgical treatment of keloid: keloid core excision. Ann Plast Surg. 2001. 46:135–140.
Article15. Lawrence WT. Treatment of earlobe keloids with surgery plus adjuvant intralesional verapamil and pressure earrings. Ann Plast Surg. 1996. 37:167–169.
Article16. Converse JM, Stallings JO. Eradication of large auricular keloids by excision, skin grafting, and intradermal injection of triamcinolone acetonide solution. Case report. Plast Reconstr Surg. 1972. 49:461–463.
Article17. Hatoko M, Kuwahara M, Shiba A, Tada H, Okazaki T, Muramatsu T, et al. Earlobe reconstruction using a subcutaneous island pedicle flap after resection of "earlobe keloid". Dermatol Surg. 1998. 24:257–261.
Article18. Berman B, Bieley HC. Keloids. J Am Acad Dermatol. 1995. 33:117–123.
Article19. Rockwell WB, Cohen IK, Ehrlich HP. Keloids and hypertrophic scars: a comprehensive review. Plast Reconstr Surg. 1989. 84:827–837.20. Friedman RM. Abnormal scars. Sel Read Plast Surg. 1995. 8:20–27.21. Ollstein RN, Siegel HW, Gillooley JF, Barsa JM. Treatment of keloids by combined surgical excision and immediate postoperative X-ray therapy. Ann Plast Surg. 1981. 7:281–285.
Article22. Norris JE. Superficial x-ray therapy in keloid management: a retrospective study of 24 cases and literature review. Plast Reconstr Surg. 1995. 95:1051–1055.23. Sclafani AP, Gordon L, Chadha M, Romo T 3rd. Prevention of earlobe keloid recurrence with postoperative corticosteroid injections versus radiation therapy: a randomized, prospective study and review of the literature. Dermatol Surg. 1996. 22:569–574.
Article24. Stashower ME. Successful treatment of earlobe keloids with imiquimod after tangential shave excision. Dermatol Surg. 2006. 32:380–386.
Article25. Singleton MA, Gross CW. Management of keloids by surgical excision and local injections of a steroid. South Med J. 1971. 64:1377–1381.
Article26. Kiil J. Keloids treated with topical injections of triamcinolone acetonide (kenalog). Immediate and long-term results. Scand J Plast Reconstr Surg. 1977. 11:169–172.
Article27. Barton RP. Auricular keloids: a simple method of management. Ann R Coll Surg Engl. 1978. 60:324–325.28. Salasche SJ, Grabski WJ. Keloids of the earlobes: a surgical technique. J Dermatol Surg Oncol. 1983. 9:552–556.
Article29. McCoy BJ, Diegelmann RF, Cohen IK. In vitro inhibition of cell growth, collagen synthesis, and prolyl hydroxylase activity by triamcinolone acetonide. Proc Soc Exp Biol Med. 1980. 163:216–222.
Article30. Murray JC. Scars and keloids. Dermatol Clin. 1993. 11:697–708.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bleomycin Intralesional Injection in Keloids and Hypertrophic Scars Unresponsive to Previous Corticosteroid Intralesional Injection and/or Laser Treatment: A Case Series and Review of the Literature
- A Comparative Study on Recurrence of Earlobe Keloids after Postoperative Adjuvant Therapy
- Intralesional Cryosurgery for the Treatment of Earlobe Keloid
- Earlobe Keloid Treated by Autograft after Excision and Immediate Corticosteroid Intrawound Injection
- Pilot Study of the Efficacy of 578 nm Copper Bromide Laser Combined with Intralesional Corticosteroid Injection for Treatment of Keloids and Hypertrophic Scars
