Ann Dermatol.
2014 Oct;26(5):559-563. 10.5021/ad.2014.26.5.559.
Different Anatomical Distribution of Basal Cell Carcinoma Subtypes in Iranian Population: Association between Site and Subtype
- Affiliations
-
- 1Department of Dermatopathology, Razi Hospital, Tehran University of Medical Sciences, Tehran, Iran.
- 2Department of Dermatology, Shahid Beheshti University of Medical Science, Tehran, Iran.
- 3Department of Internal Medicine, Shahid Beheshti University of Medical Science, Tehran, Iran.
- 4Department of Dermatology, University of California San Francisco, San Francisco, CA, USA.
- 5Department of Pathology, Tehran University of Medical Sciences, Tehran, Iran. aabbasi@razi.tums.ac.ir
- KMID: 2265487
- DOI: http://doi.org/10.5021/ad.2014.26.5.559
Abstract
- BACKGROUND
Basal cell carcinoma (BCC) is the most common type of human cancer. Despite the high prevalence of these tumors, there is a lack of reliable epidemiological data in some regions including Iran.
OBJECTIVE
To assess the relationship between BCC subtypes and anatomical distribution in the Iranian population.
METHODS
There were 876 patients with a single BCC enrolled in this study (March 2007 to March 2010; Razi Dermatology Center, Tehran, Iran).
RESULTS
Among 876 patients, 544 were males and 332 females. Of the lesions, 43% were nodular, 32.4% mixed type, 3% superficial and rest of other subtypes. In the lesion location, 58.2% were on the face, 29.2% on scalp, 6.2% on ears, 2.3% on neck, 1.7% on trunk and 1.3% on the extremities. There was no significant difference between male and female in the BCC subtypes, but anatomical distribution of the tumor was different (p=0.002). Most of the trunk-arising BCCs were superficial, and most of the facial BCCs were nodular subtype. Also, most of the BCC subtypes occurred in patients between 40 to 80 years old and mostly on the face and scalp (p=0.04). However, superficial BCCs mostly occurred in younger patients over others (p=0.001).
CONCLUSION
Subtype is associated with a site, independent of gender or age. Also BCCs occurring on the trunk are mostly of the superficial subtype.
Figure
-
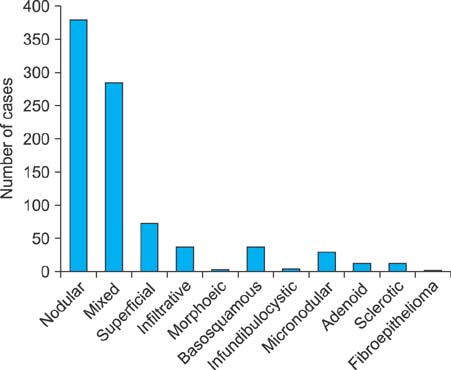
Fig. 1 Different subtypes of tumor.
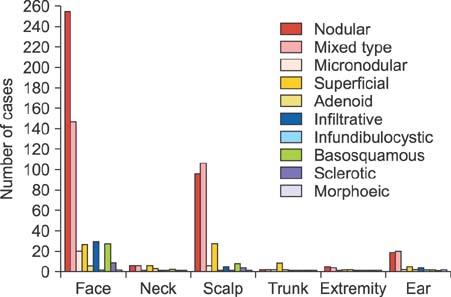
Fig. 2 Histologic subtypes of basal cell carcinomas within topographic regions (n=876).
Reference
-
1. Tiftikcioğlu YO, Karaaslan O, Aksoy HM, Aksoy B, Koçer U. Basal cell carcinoma in Turkey. J Dermatol. 2006; 33:91–95.
Article2. Rippey JJ. Why classify basal cell carcinomas? Histopathology. 1998; 32:393–398.
Article3. Ghafouri-Fard S, Abbasi A, Moslehi H, Faramarzi N, Taba Taba, Mobasheri MB, et al. Elevated expression levels of testis-specific genes TEX101 and SPATA19 in basal cell carcinoma and their correlation with clinical and pathological features. Br J Dermatol. 2010; 162:772–779.
Article4. Wong CS, Strange RC, Lear JT. Basal cell carcinoma. BMJ. 2003; 327:794–798.
Article5. Patel RV, Frankel A, Goldenberg G. An update on nonmelanoma skin cancer. J Clin Aesthet Dermatol. 2011; 4:20–27.6. Tilli CM, Van Steensel MA, Krekels GA, Neumann HA, Ramaekers FC. Molecular aetiology and pathogenesis of basal cell carcinoma. Br J Dermatol. 2005; 152:1108–1124.
Article7. Goh BK, Ang P, Wu YJ, Goh CL. Characteristics of basal cell carcinoma amongst Asians in Singapore and a comparison between completely and incompletely excised tumors. Int J Dermatol. 2006; 45:561–564.
Article8. Raasch BA, Buettner PG, Garbe C. Basal cell carcinoma: histological classification and body-site distribution. Br J Dermatol. 2006; 155:401–407.
Article9. de Vries E, Louwman M, Bastiaens M, de Gruijl F, Coebergh JW. Rapid and continuous increases in incidence rates of basal cell carcinoma in the southeast Netherlands since 1973. J Invest Dermatol. 2004; 123:634–638.
Article10. Scrivener Y, Grosshans E, Cribier B. Variations of basal cell carcinomas according to gender, age, location and histopathological subtype. Br J Dermatol. 2002; 147:41–47.
Article11. Bastiaens MT, Hoefnagel JJ, Bruijn JA, Westendorp RG, Vermeer BJ, Bouwes Bavinck JN. Differences in age, site distribution, and sex between nodular and superficial basal cell carcinoma indicate different types of tumors. J Invest Dermatol. 1998; 110:880–884.
Article12. Heckmann M, Zogelmeier F, Konz B. Frequency of facial basal cell carcinoma does not correlate with site-specific UV exposure. Arch Dermatol. 2002; 138:1494–1497.
Article13. Morison WL. Recent advances in phototherapy and photochemotherapy of skin disease. J Dermatol Sci. 1990; 1:141–147.
Article14. Jaramillo-Ayerbe F. Cryosurgery in difficult to treat basal cell carcinoma. Int J Dermatol. 2000; 39:223–229.
Article15. Reizner GT, Chuang TY, Elpern DJ, Stone JL, Farmer ER. Basal cell carcinoma in Kauai, Hawaii: the highest documented incidence in the United States. J Am Acad Dermatol. 1993; 29:184–189.
Article16. Koh D, Wang H, Lee J, Chia KS, Lee HP, Goh CL. Basal cell carcinoma, squamous cell carcinoma and melanoma of the skin: analysis of the Singapore Cancer Registry data 1968-97. Br J Dermatol. 2003; 148:1161–1166.
Article17. van Dam RM, Huang Z, Rimm EB, Weinstock MA, Spiegelman D, Colditz GA, et al. Risk factors for basal cell carcinoma of the skin in men: results from the health professionals follow-up study. Am J Epidemiol. 1999; 150:459–468.
Article18. McCormack CJ, Kelly JW, Dorevitch AP. Differences in age and body site distribution of the histological subtypes of basal cell carcinoma. A possible indicator of differing causes. Arch Dermatol. 1997; 133:593–596.
Article19. Turhan-Haktanir N, Dilek FH, Demir Y, Sahin O. Presence of interferon regulatory factor-1 in aggressive and nonaggressive histological variants of Basal cell carcinoma specimens. J Cutan Aesthet Surg. 2010; 3:34–37.
Article20. Cohen PR, Schulze KE, Nelson BR. Cutaneous carcinoma with mixed histology: a potential etiology for skin cancer recurrence and an indication for Mohs microscopically controlled surgical excision. South Med J. 2005; 98:740–747.
Article21. Cohen PR, Schulze KE, Nelson BR. Basal cell carcinoma with mixed histology: a possible pathogenesis for recurrent skin cancer. Dermatol Surg. 2006; 32:542–551.
Article22. Betti R, Radaelli G, Mussino F, Menni S, Crosti C. Anatomic location and histopathologic subtype of basal cell carcinomas in adults younger than 40 or 90 and older: any difference? Dermatol Surg. 2009; 35:201–206.
Article23. Roudier-Pujol C, Auperin A, Nguyen T, Duvillard P, Benhamou E, Avril M. Basal cell carcinoma in young adults: not more aggressive than in older patients. Dermatology. 1999; 199:119–123.
Article24. Cox NH. Basal cell carcinoma in young adults. Br J Dermatol. 1992; 127:26–29.
Article25. Lovatt TJ, Lear JT, Bastrilles J, Wong C, Griffiths CE, Ramachandran S, et al. Associations between UVR exposure and basal cell carcinoma site and histology. Cancer Lett. 2004; 216:191–197.
Article26. Yap FB. Clinical characteristics of basal cell carcinoma in a tertiary hospital in Sarawak, Malaysia. Int J Dermatol. 2010; 49:176–179.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Features of Basal Cell Carcinoma according to Histological Subtype
- Distribution of Histologic Subtypes of Basal Cell Carcinoma by Facial Aesthetic Unit and Subunit
- Clinicohistopathological Study of Recurrent Basal Cell Carcinomas after Surgical Excision
- Comparative Analysis of Squamous Cell Differentiation by Histologic Subtypes in Basal Cell Carcinoma
- A Case of Multiple Basal Cell Carcinomas in Nevoid Basal Cell Carcinoma Syndrome
