J Gynecol Oncol.
2009 Jun;20(2):86-90. 10.3802/jgo.2009.20.2.86.
Role of high risk-human papilloma virus test in the follow-up of patients who underwent conization of the cervix for cervical intraepithelial neoplasia
- Affiliations
-
- 1Department of Obstetrics and Gynecology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea.
- 2Center for Uterine Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Korea. ssseomd@ncc.re.kr
- 3Cancer Biostatistics Branch, Research Institute and Hospital, National Cancer Center, Goyang, Korea.
- KMID: 2245089
- DOI: http://doi.org/10.3802/jgo.2009.20.2.86
Abstract
OBJECTIVE
To examine whether the presence of high risk-human papilloma virus (HR-HPV) after conization of the cervix was a risk factor for persistence or recurrence of cervical intraepithelial neoplasia (CIN) and whether HR-HPV test could be a guideline for post-therapy surveillance.
METHODS
The study retrospectively analyzed data from 243 patients who underwent LLETZ or CKC of the cervix due to CIN.
RESULTS
A positive HR-HPV test result which was performed between 3 and 6 months after procedure was a risk factor for persistent or recurrent cytological (p<0.001, odds ratio [OR]=22.51, 95% confidence interval [CI]=9.74-52.02) and pathological (p<0.001, OR=18.28, 95% CI=5.55-60.20) abnormalities.
CONCLUSION
HR-HPV positive patients between 3 and 6 months after procedure should undergo frequent and meticulous post-therapy surveillance, while HR-HPV negative patients do not require such high-level surveillance and could undergo routine surveillance.
Keyword
MeSH Terms
Figure
-
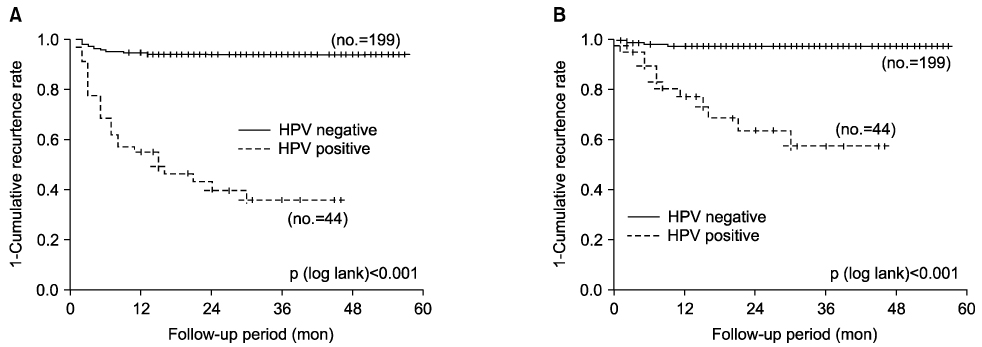
Fig. 1 Persistent or recurrent (A) cytological (left, p<0.001) or (B) pathological (right, p<0.001) abnormalities according to HR-HPV test results between 3 and 6 months after LLETZ or CKC. HR-HPV: high risk-human papilloma virus, LLETZ: large loop excision of transformation zone, CKC: cold knife conization.
Reference
-
1. Kucera E, Sliutz G, Czerwenka K, Breitenecker G, Leodolter S, Reinthaller A. Is high-risk human papillomavirus infection associated with cervical intraepithelial neoplasia eliminated after conization by large-loop excision of the transformation zone? Eur J Obstet Gynecol Reprod Biol. 2001. 100:72–76.2. Nagai Y, Maehama T, Asato T, Kanazawa K. Persistence of human papillomavirus infection after therapeutic conization for CIN 3: is it an alarm for disease recurrence? Gynecol Oncol. 2000. 79:294–299.3. Soutter WP, de Barros Lopes A, Fletcher A, Monaghan JM, Duncan ID, Paraskevaidis E, et al. Invasive cervical cancer after conservative therapy for cervical intraepithelial neoplasia. Lancet. 1997. 349:978–980.4. Husseinzadeh N, Shbaro I, Wesseler T. Predictive value of cone margins and post-cone endocervical curettage with residual disease in subsequent hysterectomy. Gynecol Oncol. 1989. 33:198–200.5. Jones HW 3rd, Buller RE. The treatment of cervical intraepithelial neoplasia by cone biopsy. Am J Obstet Gynecol. 1980. 137:882–886.6. Lapaquette TK, Dinh TV, Hannigan EV, Doherty MG, Yandell RB, Buchanan VS. Management of patients with positive margins after cervical conization. Obstet Gynecol. 1993. 82:440–443.7. Lin H, Chang HY, Huang CC, Changchien CC. Prediction of disease persistence after conization for microinvasive cervical carcinoma and cervical intraepithelial neoplasia grade 3. Int J Gynecol Cancer. 2004. 14:311–316.8. Livasy CA, Maygarden SJ, Rajaratnam CT, Novotny DB. Predictors of recurrent dysplasia after a cervical loop electrocautery excision procedure for CIN-3: a study of margin, endocervical gland, and quadrant involvement. Mod Pathol. 1999. 12:233–238.9. Lu CH, Liu FS, Tseng JJ, Ho ES. Predictive factors for residual disease in subsequent hysterectomy following conization for CIN III. Gynecol Oncol. 2000. 79:284–288.10. Moore BC, Higgins RV, Laurent SL, Marroum MC, Bellitt P. Predictive factors from cold knife conization for residual cervical intraepithelial neoplasia in subsequent hysterectomy. Am J Obstet Gynecol. 1995. 173:361–366. discussion 6-8.11. Paterson-Brown S, Chappatte OA, Clark SK, Wright A, Maxwell P, Taub NA, et al. The significance of cone biopsy resection margins. Gynecol Oncol. 1992. 46:182–185.12. Phelps JY 3rd, Ward JA, Szigeti J 2nd, Bowland CH, Mayer AR. Cervical cone margins as a predictor for residual dysplasia in post-cone hysterectomy specimens. Obstet Gynecol. 1994. 84:128–130.13. Paraskevaidis E, Koliopoulos G, Alamanos Y, Malamou-Mitsi V, Lolis ED, Kitchener HC. Human papillomavirus testing and the outcome of treatment for cervical intraepithelial neoplasia. Obstet Gynecol. 2001. 98:833–836.14. Zielinski GD, Rozendaal L, Voorhorst FJ, Berkhof J, Snijders PJ, Risse EJ, et al. HPV testing can reduce the number of follow-up visits in women treated for cervical intraepithelial neoplasia grade 3. Gynecol Oncol. 2003. 91:67–73.15. Houfflin Debarge V, Collinet P, Vinatier D, Ego A, Dewilde A, Boman F, et al. Value of human papillomavirus testing after conization by loop electrosurgical excision for high-grade squamous intraepithelial lesions. Gynecol Oncol. 2003. 90:587–592.16. Almog B, Gamzu R, Bornstein J, Levin I, Fainaru O, Niv J, et al. Clinical and economic benefit of HPV-load testing in follow-up and management of women postcone biopsy for CIN2-3. Br J Cancer. 2003. 89:109–112.17. Nobbenhuis MA, Meijer CJ, van den Brule AJ, Rozendaal L, Voorhorst FJ, Risse EK, et al. Addition of high-risk HPV testing improves the current guidelines on follow-up after treatment for cervical intraepithelial neoplasia. Br J Cancer. 2001. 84:796–801.18. Lin CT, Tseng CJ, Lai CH, Hsueh S, Huang KG, Huang HJ, et al. Value of human papillomavirus deoxyribonucleic acid testing after conization in the prediction of residual disease in the subsequent hysterectomy specimen. Am J Obstet Gynecol. 2001. 184:940–945.19. Jain S, Tseng CJ, Horng SG, Soong YK, Pao CC. Negative predictive value of human papillomavirus test following conization of the cervix uteri. Gynecol Oncol. 2001. 82:177–180.20. Bar-Am A, Gamzu R, Levin I, Fainaru O, Niv J, Almog B. Follow-up by combined cytology and human papillomavirus testing for patients post-cone biopsy: results of a long-term follow-up. Gynecol Oncol. 2003. 91:149–153.21. Negri G, Gampenrieder J, Vigl EE, Haitel A, Menia E, Mian C. Human papilloma virus typing at large loop excision of the transformation zone of the cervix uteri. Anticancer Res. 2003. 23:4289–4292.22. Chua KL, Hjerpe A. Human papillomavirus analysis as a prognostic marker following conization of the cervix uteri. Gynecol Oncol. 1997. 66:108–113.23. Park JY, Lee SM, Yoo CW, Kang S, Park SY, Seo SS. Risk factors predicting residual disease in subsequent hysterectomy following conization for cervical intraepithelial neoplasia (CIN) III and microinvasive cervical cancer. Gynecol Oncol. 2007. 107:39–44.24. Park JY, Lee KH, Dong SM, Kang S, Park SY, Seo SS. The association of pre-conization high-risk HPV load and the persistence of HPV infection and persistence/recurrence of cervical intraepithelial neoplasia after conization. Gynecol Oncol. 2008. 108:549–554.25. Wright TC Jr, Cox JT, Massad LS, Carlson J, Twiggs LB, Wilkinson EJ. 2001 consensus guidelines for the management of women with cervical intraepithelial neoplasia. Am J Obstet Gynecol. 2003. 189:295–304.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- ERRATUM: Role of high risk-human papilloma virus test in the follow-up of patients who underwent conization of the cervix for cervical intraepithelial neoplasia
- Diagnostic and Therapeutic Significance of Conization of the Cervix in Patients with Cervical Intraepithelial Neoplasm
- Follow-up of Cervical Intraepithelial Neoplasia after Conization: The Clinical Usefulness of Repeat Conization
- Loop diathermy and cold-knife conization in patients with cervical intraepithelial neoplasia: a comparative study
- Cytologic Smear to Evaluate the Endocervical Canal after Cervical Conization
