Additional Breast Ultrasound Examinations in Clustered Calcifications: for Improving Diagnostic Performance
- Affiliations
-
- 1Department of Radiology, Korea University Ansan Hospital, Ansan, Korea. seoboky@korea.ac.kr
- 2Department of Biostatistics, Korea University College of Medicine, Seoul, Korea.
- 3Department of Radiology, Korea University Anam Hospital, Seoul, Korea.
- 4Department of Radiology, Korea University Guro Hospital, Seoul, Korea.
- 5Department of General Surgery, Korea University Ansan Hospital, Ansan, Korea.
- 6Department of General Surgery, Korea University Anam Hospital, Seoul, Korea.
- KMID: 2242004
- DOI: http://doi.org/10.4048/jbc.2009.12.3.142
Abstract
- PURPOSE
We wanted to determine whether additional breast ultrasound examinations are needed for patients who have clustered calcifications found by mammography for the detection of breast carcinomas.
METHODS
We performed targeted ultrasound examinations in 125 consecutive patients who had clustered calcifications found by mammography. Forty-eight pathologically proven patients with 61 breast lesions were included in this study (26 invasive carcinomas, 10 ductal carcinomas in situ and 25 benign diseases). Two breast radiologists evaluated the mammography and the ultrasound findings and they graded the probability of malignancy by consensus as follows: definitely benign 1, probably benign 2, probably malignant 3, and definitely malignant 4. The diagnostic performance values, including the sensitivity, specificity, accuracy, positive predictive value and negative predictive value, for mammography and additional ultrasound were compared using McNemar's test and receiver operating characteristic (ROC) analysis. On the ROC analysis, areas under the ROC curves (AUC) and 95% confidence intervals (CI) were obtained.
RESULTS
The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value for making the diagnosis of breast carcinoma by mammography were 88.9%, 12.0%, 57.4%, 59.3%, and 42.9% and those for additional ultrasound were 94.4%, 64.0%, 82.0%, 79.1%, and 88.9%, respectively. The differences of specificity and accuracy were statistically significant (p=0.0003). On the ROC analysis, ACU were significantly different between mammography (AUC=0.586, 95% CI=0.453-0.711) and ultrasound (AUC=0.823, 95% CI=0.704-0.909) (p=0.003). Clustered calcifications with associated masses or ductal changes on additional breast ultrasound had high frequency of malignancies, 79% or 73%. In addition, 87% of malignant masses were invasive carcinomas and 45% of malignant ductal changes were ductal carcinomas in situ.
CONCLUSION
Additional breast ultrasound examinations for the lesions with clustered calcifications on mammography can improve the diagnostic performance and significantly contribute to the specificity and accuracy of a diagnosis of breast carcinoma. In addition, the ultrasound features may predict the pathologic findings such as benignity or malignancy and invasive carcinoma or ductal carcinoma in situ.
Keyword
MeSH Terms
Figure
-
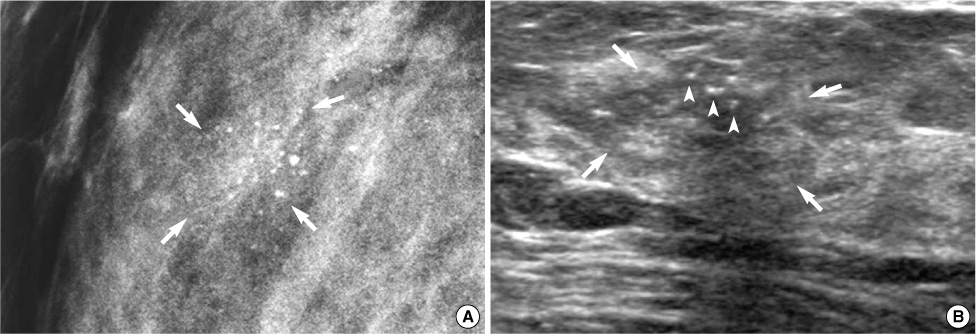
Figure 1 A 40-yr-old woman with ductal carcinoma in situ in the right breast. (A) A mediolateral oblique view showing clustered punctate calcifications (arrows) in the right breast, which were assessed as grade 2 for malignancy probability. (B) The ultrasound (US) image showing an associated indistinct irregular mass (arrows) with calcifications (arrowheads), which was assessed as grade 3 for malignancy probability. This case was false negative by mammography and true positive by breast US.
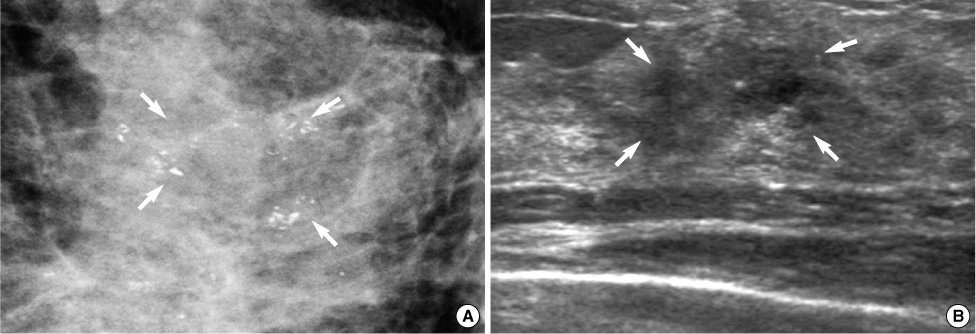
Figure 2 A 30-yr-old woman with invasive ductal carcinoma in the left breast. (A) A craniocaudal spot compression mammographic view shows clustered coarse heterogeneous calcifications (arrows) in left breast, which was assessed as grade 3. (B) A breast ultrasound (US) image demonstrates an associated mass (arrows) with an irregular shaped, spiculated margined hypoechoic pattern, which was assessed as grade 4. This case was true positive by mammography and breast US.
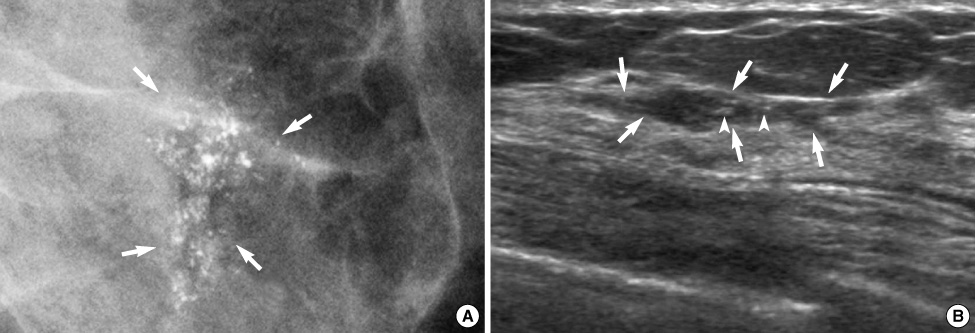
Figure 3 A 46-yr-old woman with ductal carcinoma in situ in the left breast. (A) Mediolateral oblique view shows clustered fine pleomorphic calcifications (arrows) in the left breast. Malignancy probability was assessed as grade 4 on mammography. (B) A breast ultrasound (US) image shows associated ductal changes (arrows) with calcifications (arrowheads). On ultrasound, the malignancy probability was assessed as grade 3. This lesion was true positive by mammography and breast US.
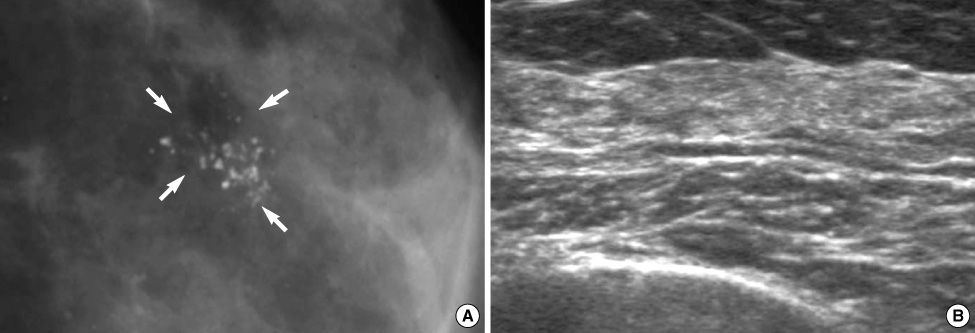
Figure 4 A 48-yr-old woman with nonproliferative fibrocystic change in the left breast. (A) A mediolateral oblique view shows clustered fine pleomorphic calcifications (arrows) in the left breast, which were assessed as grade 3 for malignancy probability. (B) A ultrasound (US) image demonstrates no abnormal finding in the region of interest, and thus the assessment was grade 1 for malignancy probability. This case was false positive by mammography and true negative by breast US.
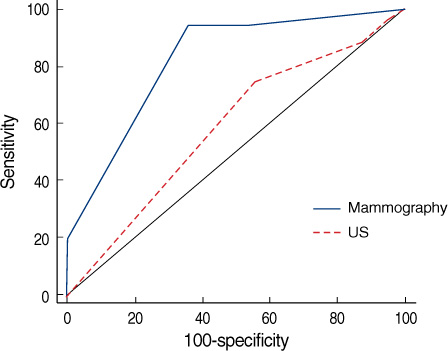
Figure 5 ROC curves for diagnostic performance of mammography and additional US. The AUC was 0.586 (95% CI, 0.453-0.711) for mammography alone and 0.823 (95% CI, 0.704-0.909) for additional breast US evaluation after mammographic examination. This difference was statistically significant (p=0.003). ROC=receiver operating characteristic; US=ultrasound; AUC=areas under the ROC curves; CI=confidence intervals.
Cited by 2 articles
-
Breast Cancer Detection in a Screening Population: Comparison of Digital Mammography, Computer-Aided Detection Applied to Digital Mammography and Breast Ultrasound
Kyu Ran Cho, Bo Kyoung Seo, Ok Hee Woo, Sung Eun Song, Jungsoon Choi, Shin Young Whang, Eun Kyung Park, Ah Young Park, Hyeseon Shin, Hwan Hoon Chung
J Breast Cancer. 2016;19(3):316-323. doi: 10.4048/jbc.2016.19.3.316.The Utility of MicroPure™ Ultrasound Technique in Assessing Grouped Microcalcifications without a Mass on Mammography
Ah Young Park, Bo Kyoung Seo, Kyu Ran Cho, Ok Hee Woo
J Breast Cancer. 2016;19(1):83-86. doi: 10.4048/jbc.2016.19.1.83.
Reference
-
1. Morimoto T, Okazaki M, Endo T. Current status and goals of mammographic screening for breast cancer in Japan. Breast Cancer. 2004. 11:73–81.
Article2. Bassett LW. Mammographic analysis of calcifications. Radiol Clin North Am. 1992. 30:93–105.3. Yang WT, Suen M, Ahuja A, Metreweli C. In vivo demonstration of microcalcification in breast cancer using high resolution ultrasound. Br J Radiol. 1997. 70:685–690.
Article4. Ciatto S, Cataliotti L, Distante V. Nonpalpable lesions detected with mammography: review of 512 consecutive cases. Radiology. 1987. 165:99–102.
Article5. Meyer JE, Eberlein TJ, Stomper PC, Sonnenfeld MR. Biopsy of occult breast lesions. Analysis of 1261 abnormalities. JAMA. 1990. 263:2341–2343.
Article6. Orel SG, Kay N, Reynolds C, Sullivan DC. BI-RADS categorization as a predictor of malignancy. Radiology. 1999. 211:845–850.
Article7. Kang SS, Ko EY, Han BK, Shin JH. Breast US in patients who had microcalcifications with low concern of malignancy on screening mammography. Eur J Radiol. 2008. 67:285–291.
Article8. Moon WK, Im JG, Koh YH, Noh DY, Park IA. US of mammographically detected clustered microcalcifications. Radiology. 2000. 217:849–854.
Article9. Cilotti A, Bagnolesi P, Moretti M, Gibilisco G, Bulleri A, Macaluso AM, et al. Comparison of the diagnostic performance of high-frequency ultrasound as a first- or second-line diagnostic tool in non-palpable lesions of the breast. Eur Radiol. 1997. 7:1240–1244.
Article10. American College of Radiology. Breast imaging reporting and data system (BI-RADS®)-Mammography. 2003. 4th ed. Reston: American College of Radiology.11. American College of Radiology. Breast imaging reporting and data system (BI-RADS®)-Ultrasound. 2003. 1st ed. Reston: American College of Radiology.12. Kasumi F. Can microcalcifications located within breast carcinomas be detected by ultrasound imaging? Ultrasound Med Biol. 1988. 14:Suppl 1. 175–182.
Article13. Chiou SY, Chou YH, Chiou HJ, Wang HK, Tiu CM, Tseng LM, et al. Sonographic features of nonpalpable breast cancer: a study based on ultrasound-guided wire-localized surgical biopsies. Ultrasound Med Biol. 2006. 32:1299–1306.
Article14. Kasumi F, Tanaka H. Jellins J, Kobayashi T, editors. Detection of microcalcifications in breast carcinoma by ultrasound. Ultrasound examination of the breast. 1983. New York: John Wiley & Sons;89–97.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnostic Utility of Artificial Intelligence in Breast Ultrasound
- Clustered Microcalcifications on Mammography: Histopathologic Correlation in Benign and Malignant Lesions
- Diagnosis of Ductal Carcinoma in situ: Role of Additional Breast Sonography
- Calcifications on Breast Ultrasonography
- Significance and diagnostic value of fine calcifications detected by mammography in female breast
