Effect of Left Atrial Decompression by Percutaneous Balloon Mitral Commissurotomy on the Atrial Electrophysiologic Properties
- Affiliations
-
- 1Cardiovascular Division, Internal Medicine, College of Medicine, Yeungnam University, Daegu, Korea. dgshin@med.yu.ac.kr
- KMID: 2227066
- DOI: http://doi.org/10.4070/kcj.2007.37.5.208
Abstract
-
BACKGROUND AND OBJECTIVES: Atrial dilatation contributes to the inducibility of atrial fibrillation (AF) by changing the atrial electrophysiological properties. There has been no report regarding the electrophysiologic data of the left atrium (LA), where the most significant electrophysiological impact might be expected to occur in case of mitral stenosis (MS). We investigated the electrophysiological changes after reduction of the LA pressure in patients who were undergoing percutaneous balloon mitral commissurotomy (PBMC).
SUBJECTS AND METHODS
We studied 26 patients (21 women, age range: 50+/-12 years) with MS, including 7 sinus rhythm (SR) patients. The effective refractory period (ERP), the monophasic action potential duration (MAPD90), and the conduction time (CT) were measured simultaneously in both atriums at 600, 500, 400 and 300 ms of drive cycle length (DCL). The restitution slope (RS) was also calculated by the S1S2 method. The atrial fibrillation cycle length (AFCL) and dominant frequency (DF) for the cases of AF were also calculated. All the measurements were repeated after PBMC.
RESULTS
The mean LA pressure was significantly reduced after PBMC in both the AF and SR patients (17.0+/-5.5 mmHg vs 10.4+/-4.0 mmHg, respectively, p<0.01, 17.6+/-7.1 mmHg vs 9.0+/-2.8 mmHg, respectively, p<0.01). A significant increase of ERP was observed in the LA after PBMC, but not in the right atrium (RA). The increase of MAPD90 after PBMC was significant in the LA at all the tested DCLs, but not in the RA. The CT was also significantly decreased at all the tested DCLs after PBMC. The RS of the LA decreased from 1.71+/-0.82 to 0.76+/-0.33 after PBMC (p=0.056). However, no significant changes of the AFCL or DF after PBMC were observed in the AF group.
CONCLUSION
Chronic atrial stretch altered the atrial electrophysiological milieu, especially in the LA, which was partially reversible in SR patients. This result supports the theoretical basis for the beneficial effects of early intervention to reduce the atrial pressure overload in MS patients.
Keyword
MeSH Terms
Figure
-

Fig. 1 ERP change after left atrial decompression. A significant increase of ERP was observed in the LA after PBMC, but not in the RA. ERP: effective refractory period at 600 ms drive cycle length, LA: left atrium, PBMC: percutaneous balloon mitral commissurotomy, RA: right atrium, NS: not significant.
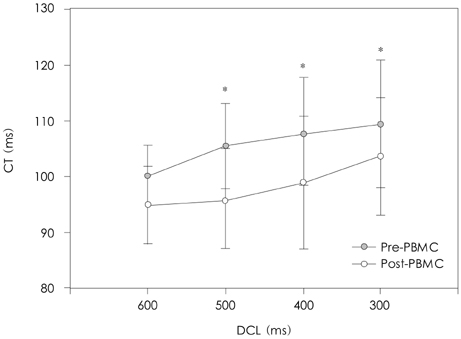
Fig. 2 Conduction time change after left atrial decompression. The CT decreased significantly at all the tested DCLs except 600 ms DCL after PBMC. CT: conduction time, DCL: drive cycle length, PBMC: percutaneous balloon mitral commissurotomy. *: p<0.05.

Fig. 3 MAP90 change after left atrial decompression. The increases of MAP90 after PBMC were significant in the LA at all the tested DCLs, but not in the RA. MAP90: 90% monophasic action potential duration at 600 ms drive cycle length, PBMC: percutaneous balloon mitral commissurotomy, LA: left atrium, RA: right atrium, DCL: drive cycle length, NS: not significant. *: p<0.05, †: p<0.01.
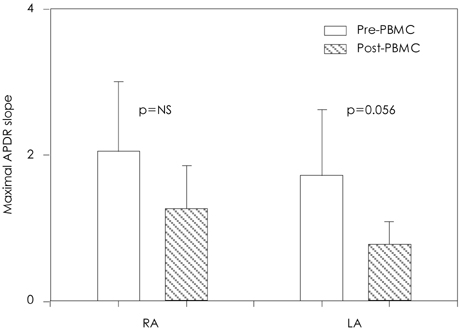
Fig. 4 Change of maximal APD restitution slope after PBMC decompression. APD: action potential duration, PBMC: percutaneous balloon mitral commissurotomy, RA: right atrium, LA: left atrium, NS: not significant.
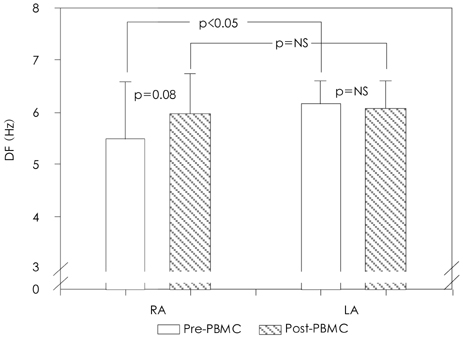
Fig. 5 Dominant frequency change after left atrial decompression. Empty bar means DF at both atrium before PBMC, and Filled bar, after PBMC. PBMC: percutaneous balloon mitral commissurotomy, DF: dominant frequency in Hz, RA: right atrium, LA: left atrium, NS: not significant.

Fig. 6 Atrial fibrillation induced by single atrial stimulation. AF induced by a single atrial stimulation (600/230 ms) in a patient with sinus rhythm during pre-PBMC. AF induction was abolished after PBMC. AF: atrial fibrillation, PBMC: percutaneous balloon mitral commissurotomy.
Reference
-
1. Kannek WB, Abbott RD, Savage DD, McNamara PM. Epidemiologic features of chronic atrial fibrillation. N Engl J Med. 1982. 306:1018–1022.2. Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA. Independent risk factor for atrial fibrillation in a population-based cohort. JAMA. 1994. 271:840–844.3. Morillo CA, Klein GJ, Jones DL, Guiraudon CM. Chronic rapid atrial pacing: structural, functional, and electrophysiological characteristics of a new model of sustained atrial fibrillation. Circulation. 1995. 91:1588–1595.4. Fareh S, Villemaire C, Nattel S. Importance of refractoriness heterogeneity in the enhanced vulnerability to atrial fibrillation induction caused by tachycardia-induced atrial electrical remodeling. Circulation. 1998. 98:2202–2209.5. Gaspo R, Bosch RF, Talajic M, Nattel S. Functional mechanisms underlying tachycardia-induced sustained atrial fibrillation in a chronic dog model. Circulation. 1997. 96:4027–4035.6. Morton JB, Byrne MJ, Power JM, Raman J, Kalman JM. Electrical remodeling of the atrium in an anatomic model of atrial flutter: relationship between substrate and triggers for conversion to atrial fibrillation. Circulation. 2002. 105:258–264.7. Kumagai K, Akimitsu S, Kawahira K, et al. Electrophysiological properties in chronic lone atrial fibrillation. Circulation. 1991. 84:1662–1668.8. Hwang GS, Kim YH, Lee HS, et al. Electrical remodeling in human atrial fibrillation influences post-cardioversion atrial mechanical dysfunction and early relapse. Korean Circ J. 1999. 29:788–795.9. Hwang GS, Kim YH, Lee HS, et al. Electrophysiologic properties of the atrium in patients with chronic and paroxysmal atrial fibrillation. Korean Circ J. 2000. 30:448–456.10. Keren G, Etzion T, Sherez J, et al. Atrial fibrillation and atrial enlargement in patients with mitral stenosis. Am Heart J. 1987. 114:1146–1155.11. Wilkins GT, Weyman AE, Abascal VM, Block PC, Palacios IF. Percutaneous balloon dilatation of the mitral valvotomy: an analysis of echocardiographic variable related to outcome and the mechanism of dilation. Br Heart J. 1988. 60:299–308.12. Franz MR, Chin MC, Sharkey HR, Griffin JC, Scheinman MM. A new single catheter technique for simultaneous measurement of action potential duration and refractory period in vivo. J Am Coll Cardiol. 1990. 16:878–886.13. Franz MR. Method and theory of monophasic action potential recording. Prog Cardiovasc Dis. 1991. 33:347–368.14. Koller ML, Riccio ML, Gilmour RF Jr. Dynamic restitution of action potential duration during electrical alternans and ventricular fibrillation. Am J Physiol. 1998. 275:H1635–H1642.15. Pak HN, Kim YH, Hwang GS, et al. Antifibrillatory and proarrhythmic effects of d,l-sotalol mediated by the action potential duration restitution kinetics. Korean Circ J. 2005. 35:282–289.16. Riccio ML, Koller ML, Gilmour RF Jr. Electrical restitution and spatiotemporal organization during ventricular fibrillation. Circ Res. 1999. 84:955–963.17. Kim KB, Rodefeld MD, Schuessler RB, Cox JL, Boineau JP. Relationship between local atrial fibrillation interval and refractory period in the isolated canine atrium. Circulation. 1996. 94:2961–2967.18. Li D, Fareh S, Leung TK, Nattel S. Promotion of atrial fibrillation by heart failure in dogs: atrial remodeling of a different sort. Circulation. 1999. 100:87–95.19. Soylu M, Demir AD, Ozdemir O, et al. Evaluation of atrial refractoriness immediately after percutaneous mitral balloon commissurotomy in patients with mitral stenosis and sinus rhythm. Am Heart J. 2004. 147:741–745.20. Sideris DA, Toumanidis ST, Thodorakis M, et al. Some observations on the mechanism of pressure related atrial fibrillation. Eur Heart J. 1994. 15:1585–1589.21. Ravelli F, Allessie M. Effects of atrial dilatation on refractory period and vulnerability to atrial fibrillation in the isolated Langenorff-perfused rabbit heart. Circulation. 1997. 96:1686–1695.22. Tse HF, Pelosi F, Oral H, Knight BP, Strickberger SA, Morady F. Effects of simultaneous atrioventricular pacing on atrial refractoriness and atrial fibrillation inducibility: role of atrial mechanoelectrical feedback. J Cardiovasc Electrophysiol. 2001. 12:43–50.23. Calkins H, el-Atassi R, Kalbfleisch S, Langberg J, Morady F. Effects of an acute increase in atrial pressure on atrial refractoriness in humans. Pacing Clin Electrophysiol. 1992. 15:1674–1680.24. Klein LS, Miles WM, Zipes DP. Effect of atrioventricular interval during pacing or reciprocant tachycardia on atrial size, pressure, and refractory period: contraction-excitation feedback in human atrium. Circulation. 1990. 82:60–68.25. Verheule S, Wilson E, Everett T, Shanbhag S, Golden C, Olgin J. Alteration in atrial electrophysiology and tissue structure in a canine model of chronic atrial dilatation due to mitral regurgitation. Circulation. 2003. 107:2615–2622.26. Chen YJ, Chen SA, Tai CT, et al. Electrophysiologic characteristics of a dilated atrium in patients with paroxysmal atrial fibrillation and atrial flutter. J Interv Card Electrophysiol. 1998. 2:181–186.27. Le Grand B, Hatem S, Deroubaix E, Couetil JP, Coraboeuf E. Depressed transient outward and calcium currents in dilated human atria. Cardiovasc Res. 1994. 28:548–556.28. Moe GK, Rheinboldt WC, Abildskov JA. A computer model of atrial fibrillation. Am Heart J. 1964. 67:200–220.29. Kim YH, Pak HN, Lim SJ, et al. Role of KATP channel during sustained ventricular fibrillation: electrophysiological characteristics necessary for the inhibition and prevention of fibrillation. Korean Circ J. 2001. 31:359–369.30. Fan K, Lee KL, Chow WH, Chau E, Lau CP. Internal cardioversion of chronic atrial fibrillation during percutaneous mitral commissurotomy: insight into reversal of chronic stretch-induced atrial remodeling. Circulation. 2002. 105:2746–2752.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Balloon Valvuloplasty for Restenosis after Surgical Mitral Commissurotomy
- Change of Plasma Atrial Natriuretic Peptide(ANP) before and after Percutaneous Ballon Mitral Valvuloplasty(PMV)
- Percutaneous Mitral Balloon Valveloplasty after Successful Resolution of Left Atrial Appendage Thrombi by Oral Anticoagulation
- Assessment of Left Atrial Function Using Instantaneous Pressure-Volume Relations in Mitral Stenosis before and after Percutaneous Mitral Balloon Valvuloplasty
- Long-Term Echocardiographic follow-up of Percutaneous Mitral Balloon Valvuloplasty in Patients with Restenosis after Previous Surgical Commissurotomy
