Korean Circ J.
2012 Aug;42(8):568-570. 10.4070/kcj.2012.42.8.568.
Polyarteritis Nodosa Complicated by Chronic Total Occlusion Accompanying Aneurysms on All Coronary Arteries
- Affiliations
-
- 1Cardiovascular Division, Department of Internal Medicine, Hallym University Medical Center, Seoul, Korea. pkhmd@naver.com
- KMID: 2225009
- DOI: http://doi.org/10.4070/kcj.2012.42.8.568
Abstract
- Polyarteritis nodosa (PAN) is characterized by inflammatory necrosis of medium sized arteries. PAN can also be associated with stenosis or aneurysm of the coronary artery. However, the involvement of PAN at a coronary artery is usually asymptomatic, which makes it difficult to diagnose. In addition, all of the three main coronary arteries involved with chronic total occlusion (CTO) is a rare finding in patients with PAN. We report a patient that presented with PAN complicated by CTO and aneurysms of three main coronary arteries, without typical symptoms of angina.
MeSH Terms
Figure
-
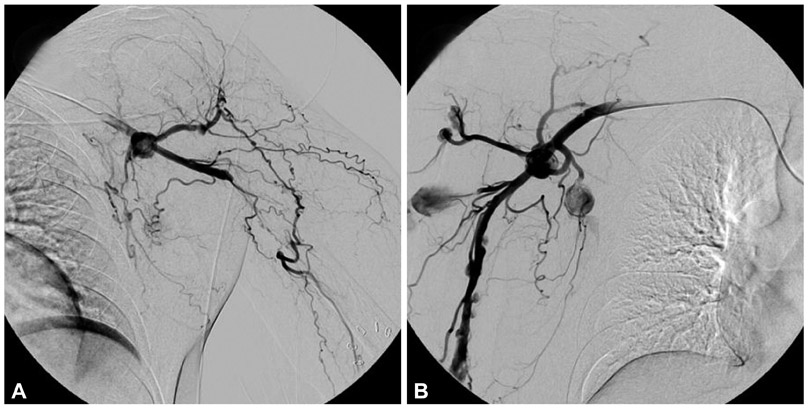
Fig. 1 The upper extremity angiography showed aneurismal change with distal total occlusion of the left axillary artery (A) and multiple aneurismal changes in the right axillary and brachial arteries (B).
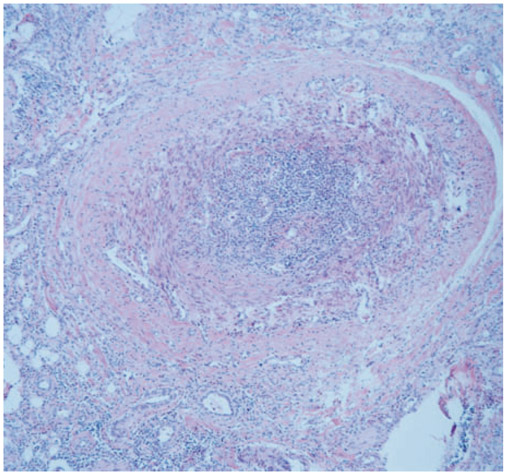
Fig. 2 Medium sized artery showed inflammation at low magnification (×100). The inflammation is especially severe in the intima and the lumen was nearly obstructed.
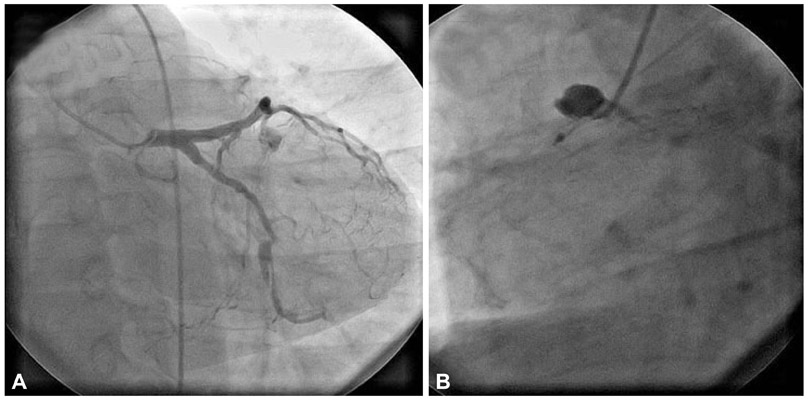
Fig. 3 The left coronary artery angiography showed a huge aneurysm and chronic total occlusion (CTO) of the left anterior descending coronary artery and the left circumflex coronary artery (A). The right coronary artery angiography revealed a huge aneurysm in its proximal segment and CTO (B).
Reference
-
1. Kastner D, Gaffney M, Tak T. Polyarteritis nodosa and myocardial infarction. Can J Cardiol. 2000. 16:515–518.2. Chu KH, Menapace FJ, Blankenship JC, Hausch R, Harrington T. Polyarteritis nodosa presenting as acute myocardial infarction with coronary dissection. Cathet Cardiovasc Diagn. 1998. 44:320–324.3. Kobayashi H, Yokoe I, Hattan N, Ohta H, Nakajima Y, Kobayashi Y. Cardiac magnetic resonance imaging in polyarteritis nodosa. J Rheumatol. 2010. 37:2427–2429.4. Pick RA, Glover MU, Vieweg WV. Myocardial infarction in a young woman with isolated coronary arteritis. Chest. 1982. 82:378–380.5. Chang HJ, Yoon YS, Kim BK, et al. Polyarteritis nodosa presenting as acute myocardial infarction. Korean Circ J. 2000. 30:227–231.6. Holsinger DR, Osmundson PJ, Edwards JE. The heart in periarteritis nodosa. Circulation. 1962. 25:610–618.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hybrid Surgery to Treat Multiple Visceral Aneurysms Secondary to Polyarteritis Nodosa
- A Case of Polyarteritis Nodosa Associated with Central Retinal Artery Occlusion
- Ischemic Pseudomembranous Colitis with Perforation due to Polyarteritis Nodosa
- A case of polyarteritis nodosa complicated by bilateral renal hematomas and U.G.I. bleeding
- A Case of Polyarteritis Nodosa Presented as Myositis
