Spontaneous Partial Regression of Coronary Artery Fistula Following Optimal Medical Therapy in a Patient Who Had Combined Significant Coronary Artery Spasm
- Affiliations
-
- 1Cardiovascular Center, Korea University Guro Hospital, Seoul, Korea. swrha617@yahoo.co.kr
- KMID: 2224936
- DOI: http://doi.org/10.4070/kcj.2013.43.5.351
Abstract
- Coronary artery fistulas (CAFs) are one of the most rare cardiac anomalies. Some patients with CAF may suffer from ischemic chest pain that originates from combined significant coronary artery spasm (CAS). Spontaneous regression of CAF has been reported in a few cases, almost all of which were infants. We report an adult patient who presented with ischemic chest pain due to multiple coronary arteries to pulmonary artery fistulas and combined significant CAS induced by intracoronary acetylcholine provocation test. Spontaneous regression of one of the fistulas was observed at 2-year angiography follow-up.
MeSH Terms
Figure
-
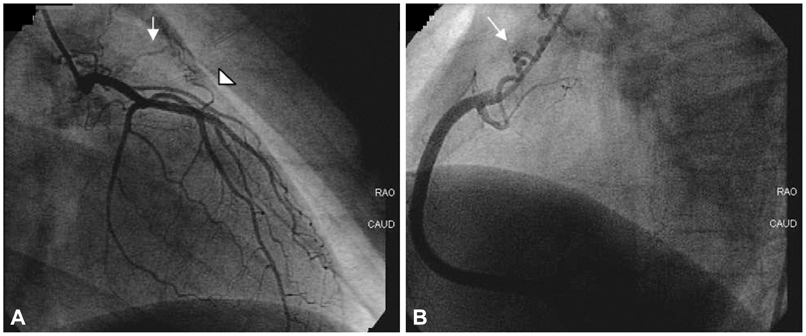
Fig. 1 Coronary arteriovenous fistulas originating from both left and right coronary arteries. A: one fistula originated from the left main (arrow), and the other from the left anterior descending artery (arrowhead). B: fistula originating from the proximal right coronary artery (arrow).
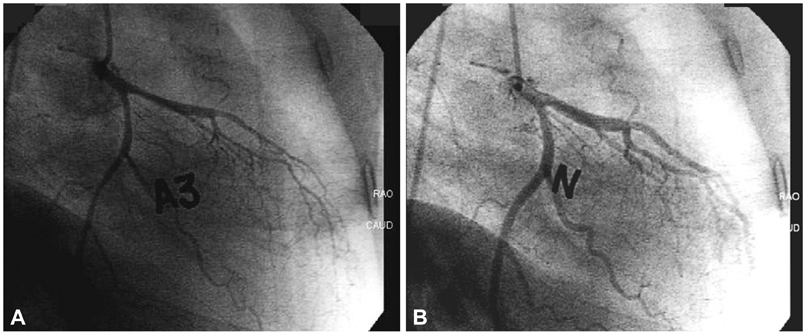
Fig. 2 The mid to distal left anterior descending artery and left circumflex artery showed significant diffuse vasoconstriction with chest pain after intracoronary acetylcholine injection (100 ug, A) which was reversed by nitroglycerin injection (200 ug, B).
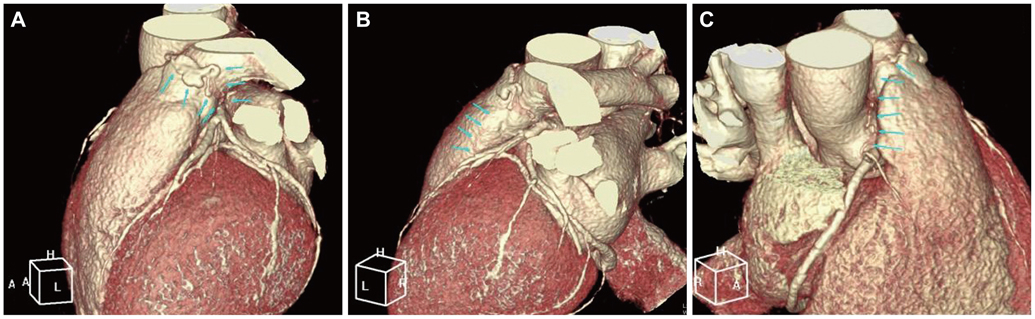
Fig. 3 Coronary multi-detector CT findings. Anomalous coronary arteriovenous fistulas from proximal left main artery to pulmonary artery (A), proximal left anterior descending artery to pulmonary artery (B), proximal right coronary artery to pulmonary artery (C).
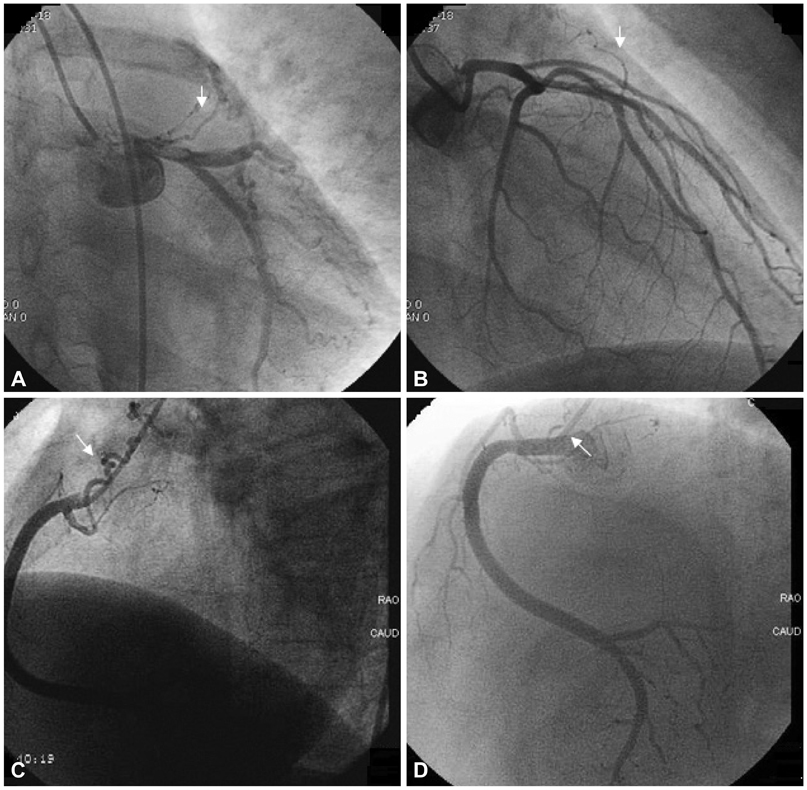
Fig. 4 Follow-up coronary angiography at two years. A and B: follow-up left coronary angiogram shows no remarkable change in both fistulas. C: previous right coronary angiogram. D: follow-up right coronary angiogram showing that the previous fistula from the right coronary artery has spontaneously regressed.
Reference
-
1. Taleb MM, Sheikh MA, Cooper CJ, Tinkel JL. Multiple coronary to pulmonary artery fistulas: a case report and review of the literature. Cardiovasc Interv Ther. 2012; 27:127–130.2. Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol. 2006; 107:7–10.3. Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation. 1978; 58:25–34.4. Umaña E, Massey CV, Painter JA. Myocardial ischemia secondary to a large coronary-pulmonary fistula--a case report. Angiology. 2002; 53:353–357.5. Bando S, Yokoi Y, Nishikado A, et al. Coronary arteriovenous fistula with vasospastic angina. Tokushima J Exp Med. 1989; 36:59–63.6. Popoiu A, Eicken A, Genz T, Schreiber C, Hess J. Regression of a coronary arterial fistula in an infant with pulmonary atresia and an intact ventricular septum. Pediatr Cardiol. 2010; 31:144–146.7. Malcić I, Belina D, Gitter R, Viljevac M, Kniewald H, Krmek N. [Spontaneous closure of fistula between right coronary artery and right ventricle in an infant]. Lijec Vjesn. 2009; 131:65–68.8. Yasuma K, Takata S, Yuasa T, et al. Bilateral coronary artery fistulas with multiple sites of drainage. Jpn Circ J. 1998; 62:783–784.9. Monmeneu JV, Bodí V, Sanchís J, et al. [Apical hypertrophic myocardiopathy and multiple fistulae between the coronary vessels and the left ventricle]. Rev Esp Cardiol. 1995; 48:768–770.10. Härle T, Kronberg K, Elsässer A. Coronary artery fistula with myocardial infarction due to steal syndrome. Clin Res Cardiol. 2012; 101:313–315.11. Kugiyama K, Yasue H, Okumura K, et al. Nitric oxide activity is deficient in spasm arteries of patients with coronary spastic angina. Circulation. 1996; 94:266–271.12. Leu HJ. Pathomorphology of vascular malformations. Analysis of 310 cases. Int Angiol. 1990; 9:147–154.13. Jaffe RB, Glancy DL, Epstein SE, Brown BG, Morrow AG. Coronary arterial-right heart fistulae. Long-term observations in seven patients. Circulation. 1973; 47:133–143.14. Nakatani S, Nanto S, Masuyama T, Tamai J, Kodama K. Spontaneous near disappearance of bilateral coronary artery-pulmonary artery fistulas. Chest. 1991; 99:1288–1289.15. Sunder KR, Balakrishnan KG, Tharakan JA, et al. Coronary artery fistula in children and adults: a review of 25 cases with long-term observations. Int J Cardiol. 1997; 58:47–53.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Native Coronary Artery and Grafted Artery Spasm Just after Coronary Artery Bypass Grafting: A Case Report
- Surgical Treatment of an Aneurysmal Coronary Artery Fistula between the Left Coronary Artery and Right Atrium: A Case Report
- Spontaneous Coronary Artery Dissection and Woven Coronary Artery: Three Cases and a Review of the Literature
- Unusual Three Cases of Adult Coronary Arteriovenous Fistula
- Three Cases of Coronary Artery Fistula from Right Coronay to Left Ventricle
