How to Achieve Complete and Permanent Pulmonary Vein Isolation without Complications
- Affiliations
-
- 1Central Utah Clinic-Cardiology, Utah Valley Regional Medical Center, Provo, UT, USA. chunhwang17@gmail.com
- 2Department of Cardiology, Dongsan Medical Center, Keimyung University, Daegu, Korea.
- KMID: 2223867
- DOI: http://doi.org/10.4070/kcj.2014.44.5.291
Abstract
- The efficacy and safety of catheter ablation for the management of atrial fibrillation (AF) has been improved in recent years. Radiofrequency (RF) catheter ablation for maintaining sinus rhythm is superior to the current antiarrhythmic drug therapy in selected patients. Pulmonary vein isolation (PVI) is the cornerstone of various catheter ablation strategies. It is well recognized that pulmonary vein (PV) antrum contributes to the AF initiation and/or perpetuation. Since PV stenosis is a complication of ablation within a PV, the ablation site for PVI has shifted to the junction between the left atrium and the PV rather than the ostium of the PV. However, PV reconnection after ablation is the major cause of recurrence of AF. The recovery of PV conduction could be caused by anatomical variations such as the failure to produce complete transmural lesion or gaps at the ablation line due to the transient electrophysiologic effects from the RF ablation. In this review, we discussed several factors to be considered for the achievement of the best PVI, including clinical aspects and technical aspects.
MeSH Terms
Figure
-

Fig. 1 Three-dimensional reconstructed images of a left atrium. A and B: the left atrium of a patient with Pectus Excavatum. A shows the relationship between the ascending aorta and the left atrial anterior wall. B shows the indentation of the anterior wall by the aorta and the flattening of the left atrium. C and D: the left atrium of a patient with Marfan syndrome, which shows significant indentation of the posterior wall by the vertebral column.
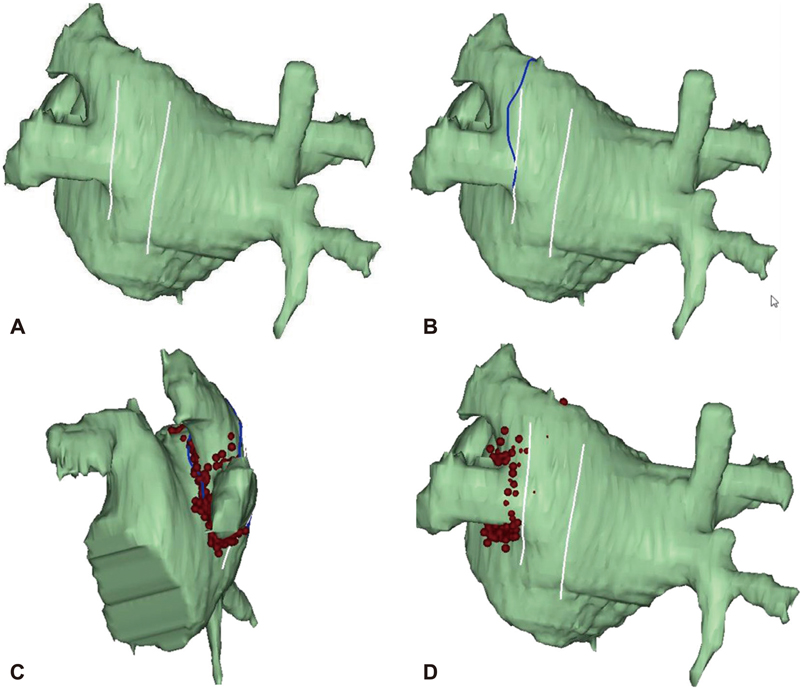
Fig. 2 The proximity of esophagus to the left pulmonary veins. The line on A shows the location of the esophagus during the CT imaging, which was located close to the ablation line (B). Continuous ablation was done in the left lateral ridge, superior, inferior, and carina of the ridge side (C). Afterwards segmental isolation of the pulmonary veins was performed following the earliest activation site of the pulmonary veins to avoid possible esophageal injury (D).
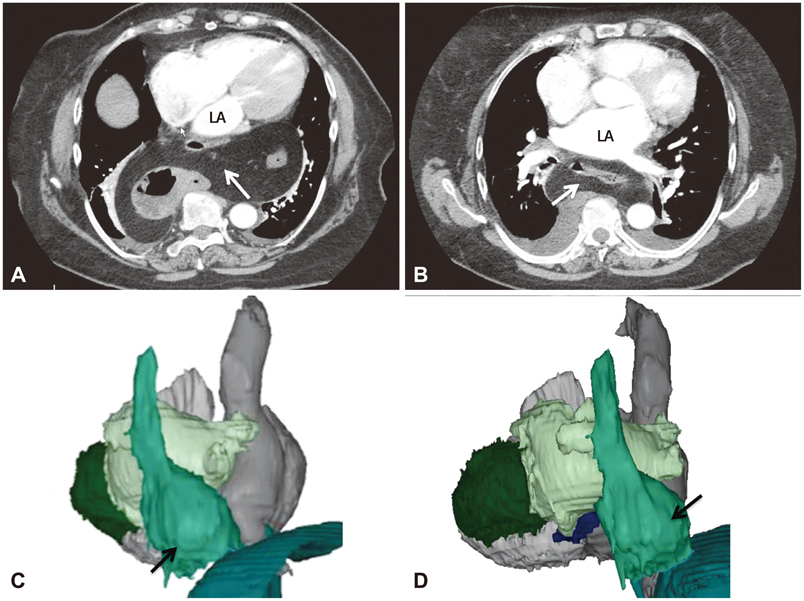
Fig. 3 Images of hiatal hernia of a stomach. A and B: the thoracic portion of the stomach (arrow) has very close contact to the posterior wall of the left atrium on CT images. C and D show 3-dimensional relationship between the herniated stomach (arrow) with the esophagus and the left atrium.
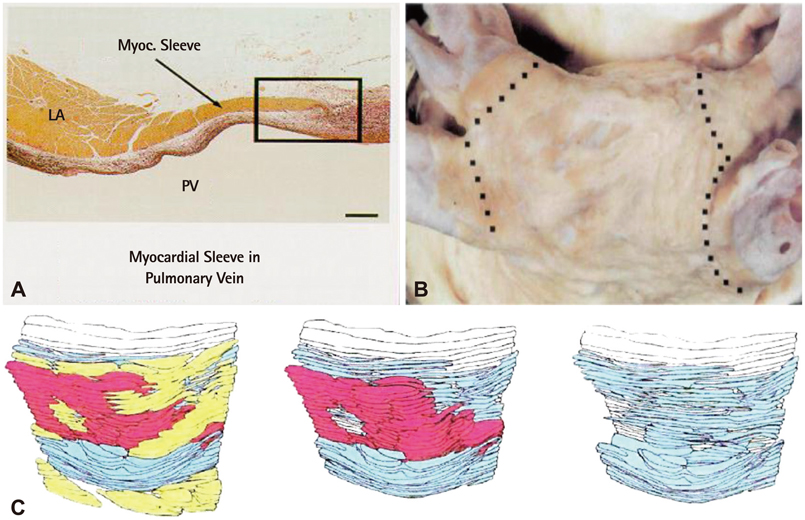
Fig. 4 Anatomical characteristics of the junction of left atrium and pulmonary vein. A: microscopic appearances of myocardial sleeves in a heart specimen. Topography of the myocardial sleeves extends along the pulmonary veins on the adventitial side. The layer of the left atrial myocardium is separated from the muscular media of the pulmonary veins by a plane of fibro-fatty tissue. B: gross appearances of myocardial sleeves around pulmonary veins. The dotted lines indicate the junction between the left atrial myocardium and the pulmonary veins revealing complete continuity. C: three-dimensional reconstruction of a cross-section, perpendicular to the long axis of part of the wall of a myocardial sleeve covering a pulmonary vein, distal to the venoatrial junction (right to left). The direction of the muscle fibers is color coded. The venoatrial junction has heterogeneous orientation of the muscle fibers (Adapted from Saito T, Waki K, Becker AE. J Cardiovasc Electrophysiol 2000;8:888-94).14)

Fig. 5 The different transseptal puncture sites depend on the right inferior pulmonary vein anatomy. A shows typical anatomy of the right inferior pulmonary vein. Bottom picture shows the location of the transseptal puncture sheaths. B shows atypical location of the right inferior pulmonary vein, which projects far posteriorly and very close to the floor of the left atrium. Bottom figure shows a modified transseptal puncture according to the variation of pulmonary vein anatomy.

Fig. 6 A shows a right anterior oblique projection. B shows a left anterior oblique projection. It shows an anteroinferior and superoposterior double transseptal puncture. The two well-separated transseptal sheaths can provide various accesses to the pulmonary veins.
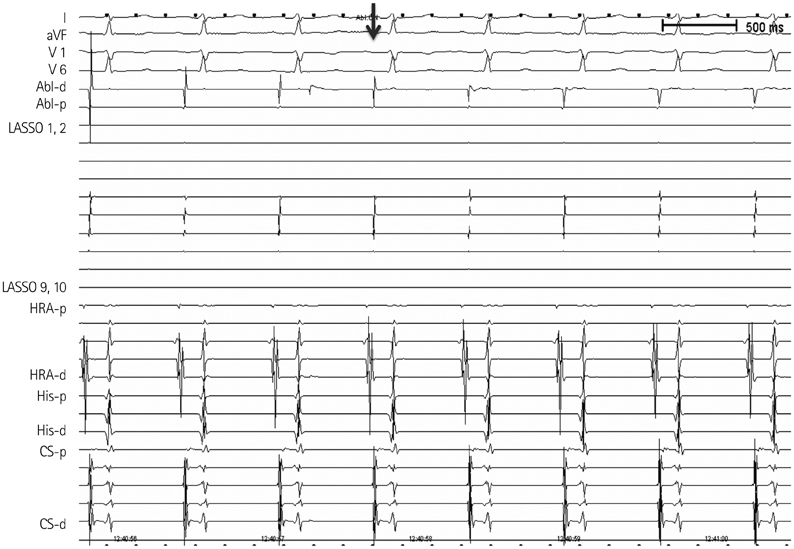
Fig. 7 Changes of electrogram by energy application. The sharp signal registered from the ablation catheter shows a loss of R wave progressively within 2 seconds after energy delivery (arrow), which implies that the catheter contact was good and the lesion formation by energy delivery was effective.
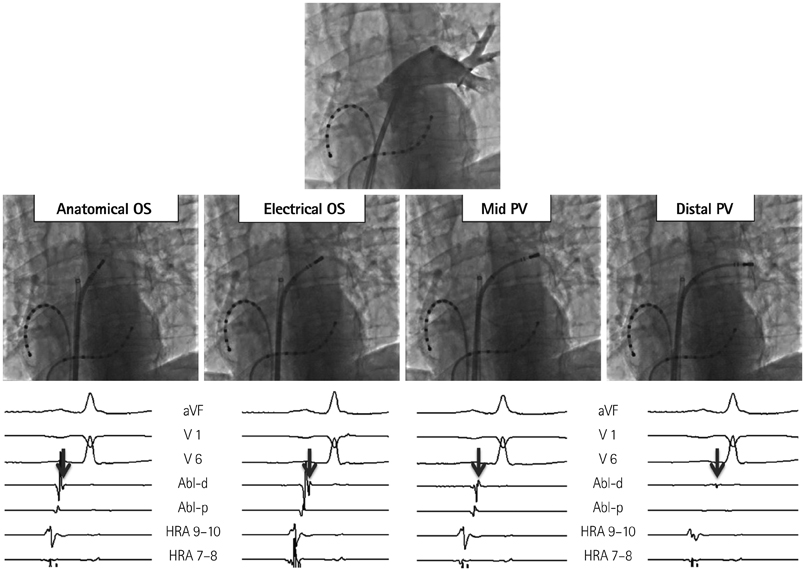
Fig. 8 Left Superior pulmonary vein mapping to identify the pulmonary vein ostium during sinus rhythm. Top picture is a left superior pulmonary venogram. Mid-row shows the location of the catheter ablation from the distal pulmonary vein to the anatomical ostium. Bottom row shows changes of the ablation electrograms according to the location. The signals from distal to mid pulmonary vein (arrows) show small single potential and later activation than the atrial activation. The signal from the electrical ostium shows high voltage multicomponent potentials with similar timing of the atrial activation. The signal of anatomical ostium has higher voltage with single component like a local atrial signal. PV: pulmonary vein, OS: ostium, Abl: ablation, HRA: high right atrium, d: distal, p: proximal.
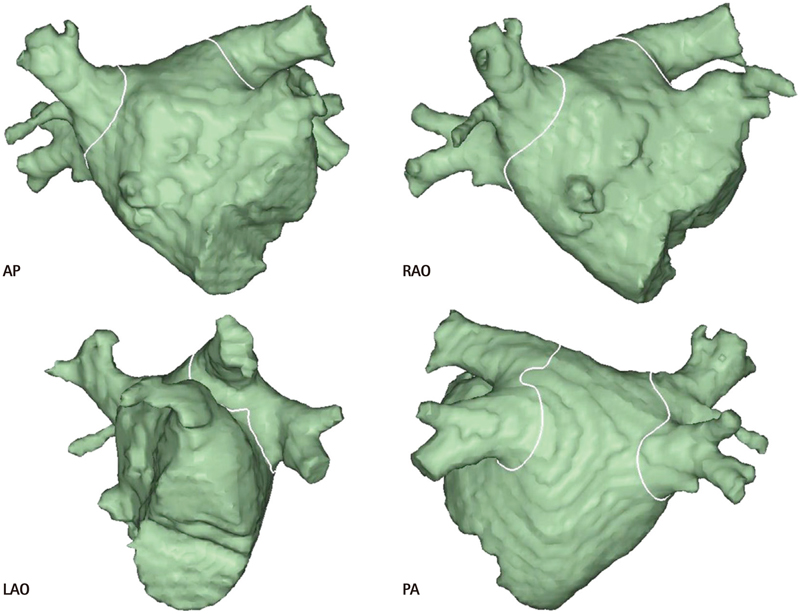
Fig. 9 Designed ablation line on the merged 3-dimensional left atrium. AP: anteroposterior projection, RAO: right anterior oblique projection, PA: posteroanterior projection, LAO: left anterior oblique projection.
Reference
-
1. Calkins H, Kuck KH, Cappato R, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Heart Rhythm. 2012; 9:632–696.2. Calkins H, Reynolds MR, Spector P, et al. Treatment of atrial fibrillation with antiarrhythmic drugs or radiofrequency ablation: two systematic literature reviews and meta-analyses. Circ Arrhythm Electrophysiol. 2009; 2:349–361.3. Piccini JP, Lopes RD, Kong MH, Hasselblad V, Jackson K, Al-Khatib SM. Pulmonary vein isolation for the maintenance of sinus rhythm in patients with atrial fibrillation: a meta-analysis of randomized, controlled trials. Circ Arrhythm Electrophysiol. 2009; 2:626–633.4. Parkash R, Tang AS, Sapp JL, Wells G. Approach to the catheter ablation technique of paroxysmal and persistent atrial fibrillation: a meta-analysis of the randomized controlled trials. J Cardiovasc Electrophysiol. 2011; 22:729–738.5. Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998; 339:659–666.6. Haïssaguerre M, Jaïs P, Shah DC, et al. Electrophysiological end point for catheter ablation of atrial fibrillation initiated from multiple pulmonary venous foci. Circulation. 2000; 101:1409–1417.7. Kalifa J, Jalife J, Zaitsev AV, et al. Intra-atrial pressure increases rate and organization of waves emanating from the superior pulmonary veins during atrial fibrillation. Circulation. 2003; 108:668–671.8. Kumagai K, Ogawa M, Noguchi H, Yasuda T, Nakashima H, Saku K. Electrophysiologic properties of pulmonary veins assessed using a multielectrode basket catheter. J Am Coll Cardiol. 2004; 43:2281–2289.9. Sanders P, Berenfeld O, Hocini M, et al. Spectral analysis identifies sites of high-frequency activity maintaining atrial fibrillation in humans. Circulation. 2005; 112:789–797.10. Lin YJ, Tsao HM, Chang SL, et al. Role of high dominant frequency sites in nonparoxysmal atrial fibrillation patients: insights from high-density frequency and fractionation mapping. Heart Rhythm. 2010; 7:1255–1262.11. Cappato R, Calkins H, Chen SA, et al. Updated worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circ Arrhythm Electrophysiol. 2010; 3:32–38.12. Arbelo E, Brugada J, Hindricks G, et al. ESC-EURObservational Research Programme: the Atrial Fibrillation Ablation Pilot Study, conducted by the European Heart Rhythm Association. Europace. 2012; 14:1094–1103.13. Hassink RJ, Aretz HT, Ruskin J, Keane D. Morphology of atrial myocardium in human pulmonary veins: a postmortem analysis in patients with and without atrial fibrillation. J Am Coll Cardiol. 2003; 42:1108–1114.14. Saito T, Waki K, Becker AE. Left atrial myocardial extension onto pulmonary veins in humans: anatomic observations relevant for atrial arrhythmias. J Cardiovasc Electrophysiol. 2000; 11:888–894.15. Tan AY, Li H, Wachsmann-Hogiu S, Chen LS, Chen PS, Fishbein MC. Autonomic innervation and segmental muscular disconnections at the human pulmonary vein-atrial junction: implications for catheter ablation of atrial-pulmonary vein junction. J Am Coll Cardiol. 2006; 48:132–143.16. McGann CJ, Kholmovski EG, Oakes RS, et al. New magnetic resonance imaging-based method for defining the extent of left atrial wall injury after the ablation of atrial fibrillation. J Am Coll Cardiol. 2008; 52:1263–1271.17. Kowalski M, Grimes MM, Perez FJ, et al. Histopathologic characterization of chronic radiofrequency ablation lesions for pulmonary vein isolation. J Am Coll Cardiol. 2012; 59:930–938.18. Ranjan R, Kato R, Zviman MM, et al. Gaps in the ablation line as a potential cause of recovery from electrical isolation and their visualization using MRI. Circ Arrhythm Electrophysiol. 2011; 4:279–286.19. Wittkampf FH, Hauer RN, Robles de Medina EO. Control of radiofrequency lesion size by power regulation. Circulation. 1989; 80:962–968.20. Jain MK, Wolf PD. Temperature-controlled and constant-power radio-frequency ablation: what affects lesion growth? IEEE Trans Biomed Eng. 1999; 46:1405–1412.21. Kautzner J, Neuzil P, Peichl P, et al. Contact force, force time integral and lesion continuity are critical to improve durable PV isolation: EFFICAS II results. Heart Rhythm. 2012; 9:S28.22. Cabrera JA, Ho SY, Climent V, Fuertes B, Murillo M, Sánchez-Quintana D. Morphological evidence of muscular connections between contiguous pulmonary venous orifices: relevance of the interpulmonary isthmus for catheter ablation in atrial fibrillation. Heart Rhythm. 2009; 6:1192–1198.23. Andrade JG, Pollak SJ, Monir G, et al. Pulmonary vein isolation using a pace-capture-guided versus an adenosine-guided approach: effect on dormant conduction and long-term freedom from recurrent atrial fibrillation--a prospective study. Circ Arrhythm Electrophysiol. 2013; 6:1103–1108.24. Sotomi Y, Inoue K, Ito N, et al. Cause of very late recurrence of atrial fibrillation or flutter after catheter ablation for atrial fibrillation. Am J Cardiol. 2013; 111:552–556.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Levoatriocardinal Vein Combined with Pulmonary Venous Varix Mimicking Arteriovenous Malformations: A Case Report
- Individual Pulmonary Vein Atresia in Adults: Report of Two Cases
- The effect of empirical superior vena cava isolation during total thoracoscopic ablation in patients with persistent atrial fibrillation
- Controlled Atrial Fibrillation after Pulmonary Vein Stenting
- Pulmonary Vein Varix: A Case Report
