Assessment of Myocardial Collateral Blood Flow with Contrast Echocardiography
- Affiliations
-
- 1Knight Cardiovascular Institute, Oregon Health & Science University, Portland, Oregon, USA. kauls@ohsu.edu
- KMID: 2223796
- DOI: http://doi.org/10.4070/kcj.2015.45.5.351
Abstract
- Humans have pre-formed collateral vessels that enlarge with ischemia. In addition, new vessels can be formed within ischemic zones from pre-formed endocardial arcades of vessels providing rich collateral flow. Collateral flow under resting conditions (if >25% of normal) is enough to maintain myocardial viability, but may be insufficient to prevent myocardial ischemia under stress. Coronary angiography is a poor tool for collateral flow assessment. Myocardial contrast echocardiography is arguably the gold standard for experimental and clinical measurement of collateral flow. This review describes several experimental and clinical studies that highlight the importance of the collateral circulation in coronary artery disease.
MeSH Terms
Figure
-
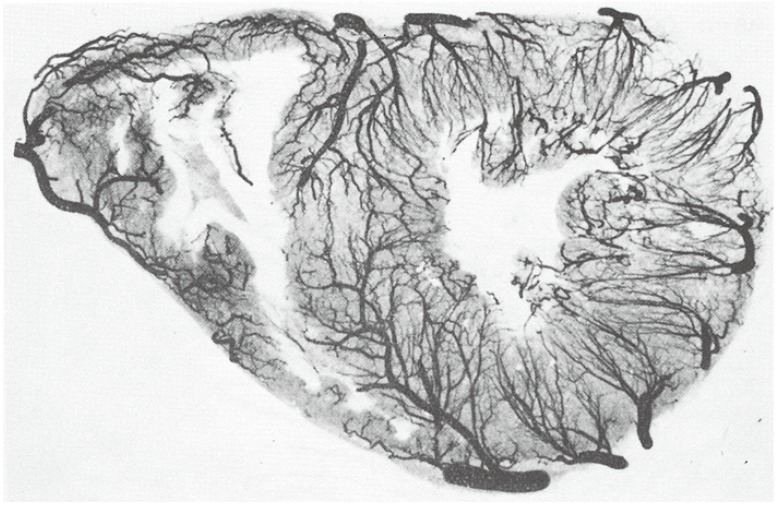
Fig. 1 Post-mortem high-resolution angiogram of a thin transverse section of the heart of a 29 year old normal individual. Note pre-existing collaterals between anterior and posterior circulations, as well as the endocardial arcades formed by the penetrating arteries. From Gross and Kugel,2) with permission from C.V. Mosby Company.

Fig. 2 Post-mortem high-resolution angiogram of a thin transverse section of the heart of an older male with left anterior descending artery occlusion, demonstrating abundant collateral vessel development within the LAD bed to circumvent infarction despite the occluded vessel. Compare with Fig. 1. From Fulton et al,3) with permission of the British Medical Association. R: right, L: left, RC: right coronary artery, LC: left circulatory artery, LCxA; left circumflex artery, ANT: left anterior descending artery, ADA: anterior diagonal artery.
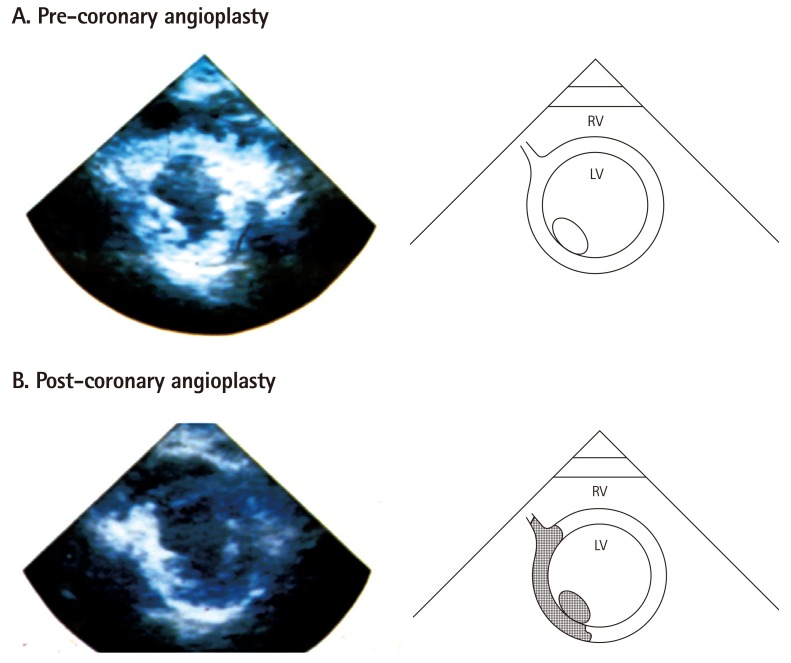
Fig. 3 Short-axis echocardiographic view of a patient with a totally occluded right coronary artery after acute myocardial infarction taken in the cardiac catheterization laboratory. A depicts a MCE image after microbubble injection into the left main coronary artery showing contrast enhancement of the entire left ventricular myocardium. B depicts the same view after successful angioplasty of the right coronary artery and direct injection of microbubbles, showing the perfusion bed of the right coronary artery. At the time of coronary occlusion, this bed was supplied by collaterals from the left system (top panel). From Sabia et al,9) with permission of the New England Medical Society. MCE: myocardial contrast echocardiography, RV: right ventricle, LV: left ventricle.
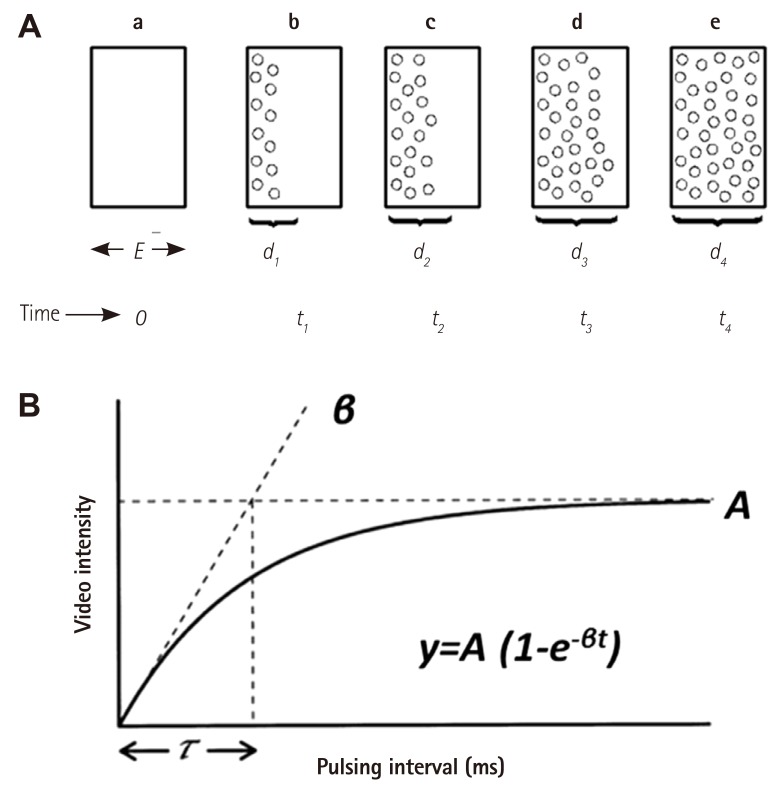
Fig. 4 Method of measuring myocardial blood flow using MCE. A shows the ultrasound beam elevation (thickness) represented as 'E' in a. If all the microbubbles in the elevation are destroyed by a single pulse of ultrasound at t0, then replenishment of the beam elevation (d1-d4, b-e), will depend on the velocity of microbubbles and time of imaging. B shows the pulsing interval (x-axis) versus video-intensity (y-axis) plot where myocardial blood volume is shown as A and rate of microbubble replenishment is shown as β. The function used to fit the relation is also depicted. Adapted from Wei et al,18) with permission of the American Heart Association. MCE: myocardial contrast echocardiography.
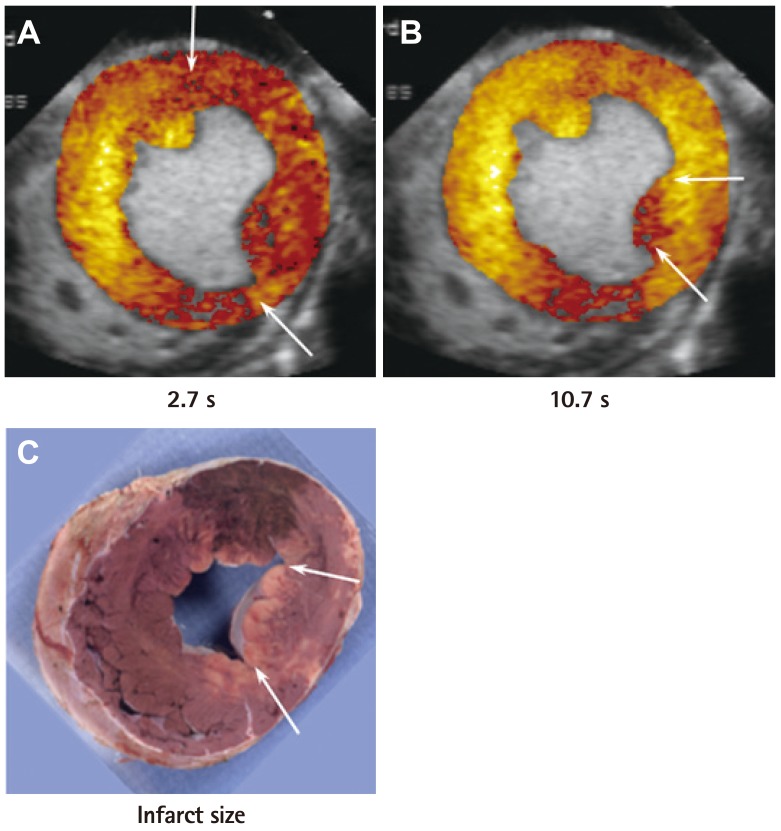
Fig. 5 Perfusion defect size at various times after bubble destruction and final infarct size (by tissue staining) in a dog undergoing 6 hours of left circumflex artery occlusion. In this example, although risk area is large (A), the infarct size is small and located at the tip of the posteromedial papillary muscle (C). This is the only region showing a perfusion defect at 10.7s when collaterals have filled the rest of the risk area (B). Adapted from Coggins et al.21) with permission of the American Heart Association.
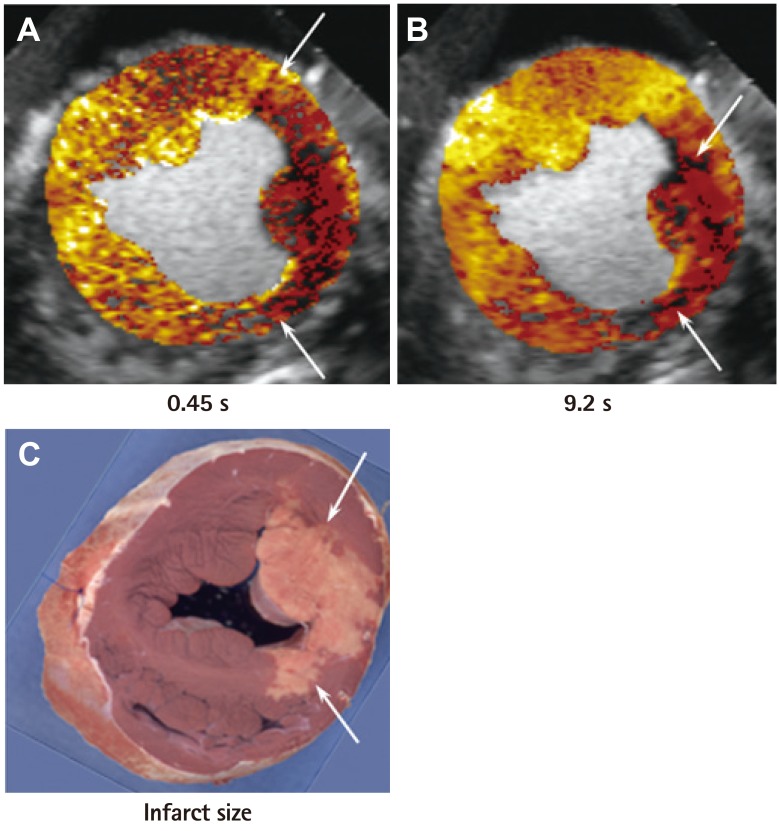
Fig. 6 Perfusion defect sizes at various times after bubble destruction and final infarct size (by tissue staining) in a dog undergoing 6 hours of left circumflex artery occlusion. In this example, although the risk area (A) is the same size as in Fig. 5, the infarct size is much larger (C) because of less collateral-derived flow. The region that became infarcted has no opacification at 9.2 s. (B) Adapted from Coggins et al.21) with permission of the American Heart Association.
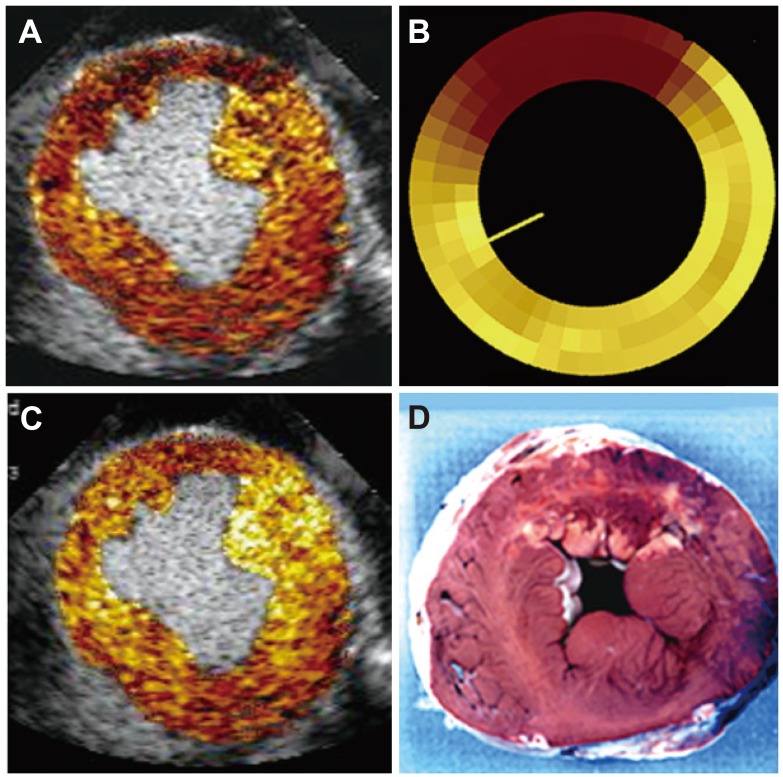
Fig. 7 Images from a dog undergoing 6 hours of left anterior descending artery occlusion with a large MCE defined risk area (A), confirmed by radiolabeled microspheres (B). The risk area is mostly filled with collateral flow several seconds later (C) resulting in a very small infarct (D). The rest of the risk area is supplied by collateral flow that is lower than in the normal remote myocardium. Thus, the circumferential extent of abnormal wall thickening was greater than the circumferential extent of infarction. MCE: myocardial contrast echocardiography.
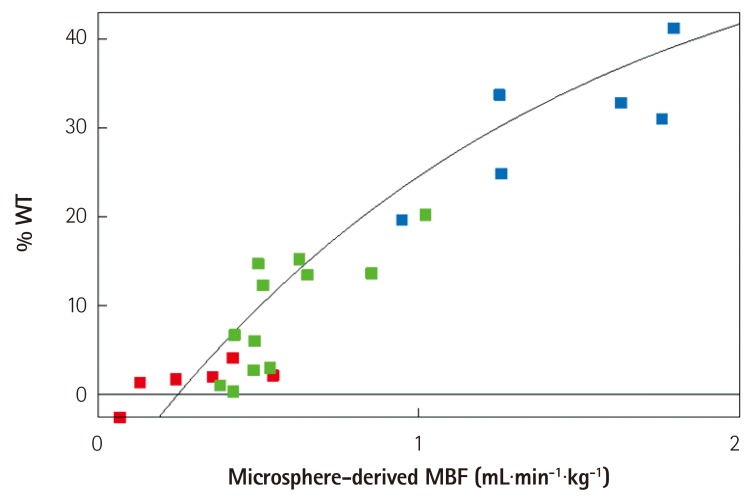
Fig. 8 Flow-function relation in dogs undergoing 6 hours of total coronary occlusion. The data points in red denote the infarcted zone, those in green denote the collateralized zone, and those in blue denote the normal myocardium. All data points fall on the same line. See text for details. From Leong-Poi et al.27) with permission of the American Heart Association. WT: wall thickening, MBF: myocardial blood flow.
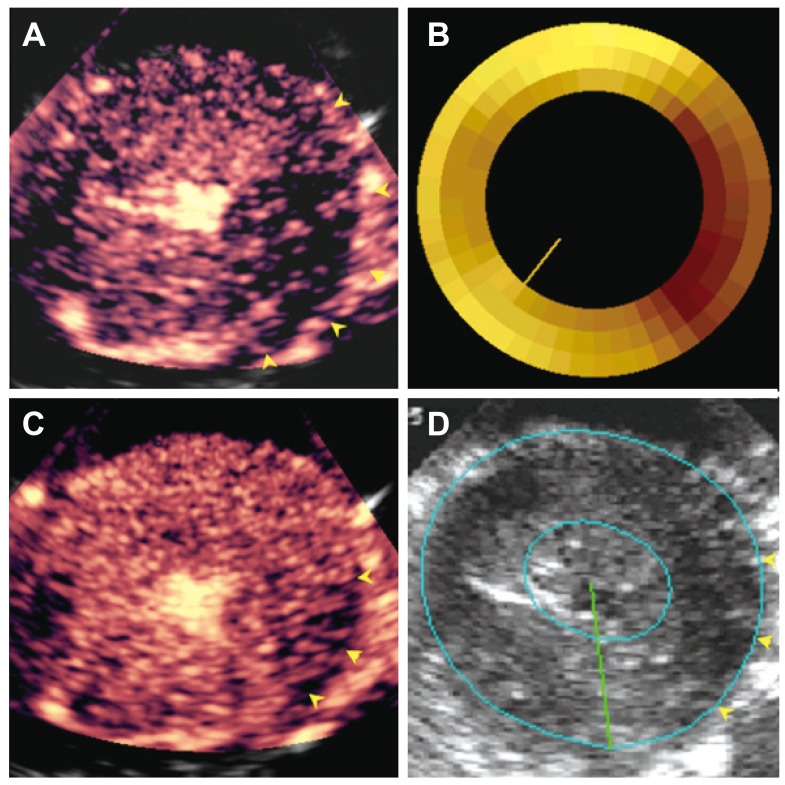
Fig. 9 Images from a dog with a non-critical single vessel left circumflex artery stenosis at peak Dobutamine dose with a large MCE-defined risk area (A) that is similar in topology to hypo-perfused zone by radiolabeled microspheres (B). The risk area is almost completely filled by collateral flow a few seconds after microbubble destruction (except for area shown by yellow arrows) (C), resulting in minimal systolic wall thickening abnormality seen on echocardiography (except for area shown by yellow arrows) (D). From Leong-Poi et al.27) with permission of the American Heart Association. MCE: myocardial contrast echocardiography.
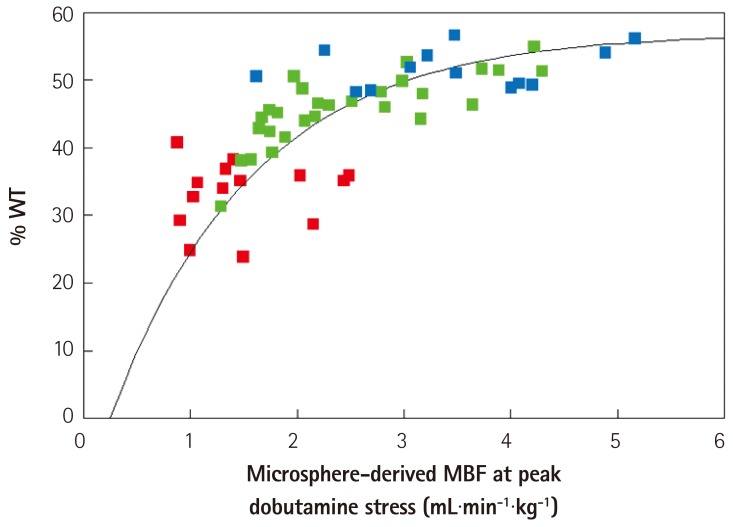
Fig. 10 Flow-function relation in dogs with non-critical single-vessel stenosis undergoing Dobutamine stress echocardiography. The data points in red denote the central portion of the perfusion defect on MCE. The data points in green are from the intermediate zone within the perfusion defect that fills with collateral flow. The data points in blue denote the remote normal myocardium. All data points fit the same curvilinear relation. At above hyperemic flows of 2-3 mL.min.g-1, wall thickening no longer increases with increase in flow. Thus, wall thickening measures during stress is not as sensitive as blood flow measurement for detection of coronary artery stenosis. See text for details. From Leong-Poi et al.27) with permission of the American Heart Association. WT: wall thickening, MBF: myocardial blood flow.
Reference
-
1. Lower R. Tractatus de corde item de motu et colore sanguinis et chli in eum transitu. KJ Franklin. Ealry Science in Oxford, Vol. 9. Oxford: Oxford University Press;1932. p. 13.2. Gross L, Kugel MA. The arterial blood vascular distribution to the left and right ventricles of the human heart. Am Heart J. 1933; 9:165–177.3. Fulton WF. Anastomotic enlargement and ischemic myocardial damage. Br Heart J. 1964; 26:1–15. PMID: 14106121.4. Baroldi G, Scomazzoni G. Coronary circulation in the normal and pathological heart. Washington, D.C.: Armed Forces Institute of Pathology;1967.5. Schaper W. Collateral Circulation: past and present. Basic Res Cardiol. 2009; 104:5–21. PMID: 19101749.6. Cohen MV. Coronary collaterals: clinical & experimental observations. Mount Kisco, N.Y.: Futura Pub. Co.;1985.7. Kaul S. Myocardial contrast echocardiography: 15 years of research and development. Circulation. 1997; 96:3745–3760. PMID: 9396479.8. Kaul S. Myocardial contrast echocardiography: a 25-year retrospective. Circulation. 2008; 118:291–308. PMID: 18625905.9. Sabia PJ, Powers ER, Ragosta M, Sarembock IJ, Burwell LR, Kaul S. An association between collateral blood flow and myocardial viability in patients with recent myocardial infarction. N Engl J Med. 1992; 327:1825–1831. PMID: 1448120.10. Sabia PJ, Powers ER, Jayaweera AR, Ragosta M, Kaul S. Functional significance of collateral blood flow in patients with recent acute myocardial infarction. A study using myocardial contrast echocardiography. Circulation. 1992; 85:2080–2089. PMID: 1591827.11. Kaul S, Gillam LD, Weyman AE. Contrast echocardiography in acute myocardial ischemia. II. The effect of site of injection of contrast agent on the estimation of area at risk for necrosis after coronary occlusion. J Am Coll Cardiol. 1985; 6:825–830. PMID: 3897342.12. Kaul S, Glasheen WP, Oliner JD, Kelly P, Gascho JA. Relation between anterograde blood flow through a coronary artery and the perfusion bed it supplies: experimental and clinical implications. J Am Coll Cardiol. 1991; 17:1403–1413. PMID: 2016458.13. Kaul S, Pandian NG, Guerrero JL, Gillam LD, Okada RD, Weyman AE. Effects of selectively altering the collateral driving pressure on regional perfusion and function in the occluded coronary bed in the dog. Circ Res. 1987; 61:77–85. PMID: 3608113.14. Vernon SM, Camarano G, Kaul S, et al. Myocardial contrast echocardiography demonstrates that collateral flow can preserve myocardial function beyond a chronically occluded coronary artery. Am J Cardiol. 1996; 78:958–960. PMID: 8888677.15. Keller MW, Segal SS, Kaul S, Duling B. The behavior of sonicated albumin microbubbles within the microcirculation: a basis for their use during myocardial contrast echocardiography. Circ Res. 1989; 65:458–467. PMID: 2752551.16. Jayaweera AR, Edwards N, Glasheen WP, Villanueva FS, Abbott RD, Kaul S. In vivo myocardial kinetics of air-filled albumin microbubbles during myocardial contrast echocardiography. Comparison with radiolabeled red blood cells. Circ Res. 1994; 74:1157–1165. PMID: 8187282.17. Wei K, Skyba DM, Firschke C, Jayaweera AR, Lindner JR, Kaul S. Interactions between microbubbles and ultrasound: in vitro and in vivo observations. J Am Coll Cardiol. 1997; 29:1081–1088. PMID: 9120163.18. Wei K, Jayaweera AR, Firoozan S, Linka A, Skyba DM, Kaul S. Quantification of myocardial blood flow with ultrasound-induced destruction of microbubbles administered as a continuous infusion. Circulation. 1998; 97:473–483. PMID: 9490243.19. Le DE, Jayaweera AR, Wei K, Coggins MP, Lindner JR, Kaul S. Changes in myocardial blood volume over a wide range of coronary driving pressures: role of capillaries beyond the autoregulation range. Heart. 2004; 90:1199–1205. PMID: 15367524.20. Lindner JR, Song J, Jayaweera AR, Sklenar J, Kaul S. Microvascular rheology of definity microbubbles after intra-arterial and intravenous administration. J Am Soc Echocardiogr. 2002; 15:396–403. PMID: 12019422.21. Coggins MP, Sklenar J, Le DE, Wei K, Lindner JR, Kaul S. Noninvasive prediction of ultimate infarct size at the time of acute coronary occlusion based on the extent and magnitude of collateralderived myocardial blood flow. Circulation. 2001; 104:2471–2477. PMID: 11705827.22. Kerber RE, Marcus ML, Ehrhardt J, Wilson R, Abboud FM. Corrrelation between echocardiographically demonstrated segmental dyskinesis and regional myocardial perfusion. Circulation. 1975; 52:1097–1104. PMID: 1182955.23. Lieberman AN, Weiss JL, Jugdutt BI, et al. Two-dimensional echocardiography and infarct size: relationship of regional wall motion and thinning to the extent of myocardial infarction in the dog. Circulation. 1981; 63:739–746. PMID: 7471327.24. Lima JA, Becker LC, Melin JA, et al. Impaired thickening of nonischemic myocardium during acute regional ischemia in the dog. Circulation. 1985; 71:1048–1059. PMID: 3986975.25. Force T, Kemper A, Perkins L, Gilfoil M, Cohen C, Parisi AF. Overestimation of infarct size by quantitative two-dimensional echocardiography: the role of tethering and of analytic procedures. Circulation. 1986; 73:1360–1368. PMID: 3698262.26. Weyman AE, Franklin TD Jr, Hogan RD, et al. Importance of temporal heterogeneity in assessing the contraction abnormalities associated with acute myocardial ischemia. Circulation. 1984; 70:102–112. PMID: 6723006.27. Leong-Poi H, Coggins MP, Sklenar J, Jayaweera AR, Wang XQ, Kaul S. Role of collateral blood flow in the apparent disparity between the extent of abnormal wall thickening and perfusion defect size during acute myocardial infarction and demand ischemia. J Am Coll Cardiol. 2005; 45:565–572. PMID: 15708705.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of collateral flow and myocardial perfusion by myocardial contrast echocardiography after coronary vasodiator during acute coronary occlusion
- Abnormal Myocardial Blood Flow Reserve Observed in Cardiac Amyloidosis
- Myocardial Contrast Echocardiography for the Assessment of Coronary Blood Flow Reserve
- Assessment of myocardial perfusion status through the angiographically visible collaterals in the ischemic heart disease
- Effect of Regional Hypoxia on Myocardial Blood Flow Through Collateral Circulation in Experimental Canine Model
