J Rheum Dis.
2012 Jun;19(3):156-159. 10.4078/jrd.2012.19.3.156.
Chronic Tophaceous Gout of the Calf Mimicking Deep Venous Thrombosis
- Affiliations
-
- 1Department of Internal Medicine, Chonbuk National University Medical School and Research Institute of Clinical Medicine, Jeonju, Korea. ywhim@jbnu.ac.kr
- KMID: 2223098
- DOI: http://doi.org/10.4078/jrd.2012.19.3.156
Abstract
- Gout is a metabolic disease characterized by hyperuricemia, recurrent attacks of acute arthritis and deposits of monosodium urate monohydrate (tophi). Gouty tophi typically deposit in the peripheral regions of the body, especially in toes and fingers. However, it can form at unusual sites and present with atypical clinical features. We here report a very rare case of patient with chronic gout who developed tophi on the calf and mimicking thrombophlebitis. She was successfully treated with drainage, colchicine and hypouricemic agents. We suggest that large tophi on the calf can be a very rare clinical feature of chronic gout and need careful attention for exact diagnosis and proper treatment.
Keyword
MeSH Terms
Figure
-
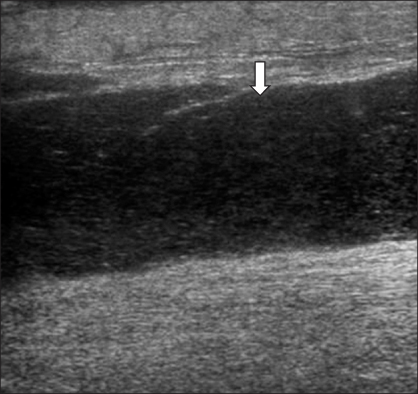
Figure 1 Ultrasonography of the left calf shows diffuse, high density on the subcutaneous layer, and a hypo-echogenic lesion between the gastrocnemius muscle and subcutaneous deep fascia (arrow).

Figure 2 T1-weighted MR images of the left calf area show a well-circumscribed, cystic lesion with low signal intensity (arrows), between the gastrocnemius muscle and the deep fascia of calf, in sagittal (A) and coronal views (B).

Figure 3 T2-weighted MR images of the left calf area show a well-circumscribed, cystic lesion with high signal intensity (arrows), between the gastrocnemius muscle and the deep fascia of the calf, in sagittal (A) and coronal views (B).
Reference
-
1. Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison's principles of internal medicine. 2008. 17th ed. New York: McGraw-Hill;2165–2167.2. Lee CH, Sung NY. The prevalence and features of Korean gout patients using the national health insurance corporation database. J Rheum Dis. 2011. 18:94–100.3. Kim EH, Jeon K, Park KW, Kim HJ, Ahn JK, Jeon CH, et al. The prevalence of gout among hyperuricemic population. J Korean Rheum Assoc. 2004. 11:7–13.4. Beers MK, Berkow R. The Merck manual of diagnosis and therapy. 2006. 18th ed. Centennial edition. West Point, Pa: Merck;768–779.5. De Yoe BE, Ng A, Miller B, Rockett MS. Peroneus brevis tendon rupture with tophaceous gout infiltration. J Foot Ankle Surg. 1999. 38:359–362.6. Yochum TR, Rowe LJ. Essentials of skeletal radiology. 2004. 3rd ed. Baltimore: Williams & Wilkins;955–968.7. Paquette S, Lach B, Guiot B. Lumbar radiculopathy secondary to gouty tophi in the filum terminale in a patient without systemic gout: case report. Neurosurgery. 2000. 46:986–988.8. Bonaldi VM, Duong H, Starr MR, Sarazin L, Richardson J. Tophaceous gout of the lumbar spine mimicking an epidural abscess: MR features. AJNR Am J Neuroradiol. 1996. 17:1949–1952.9. Bang SY, Jeong JH, Joo KB, Jun JB, Sung YK. A case of the lumbar spine involvement and sacroiliitis in a patient with gout. J Korean Rheum Assoc. 2009. 16:318–322.10. Chen CH, Chen CK, Yeh LR, Pan HB, Yang CF. Intra-abdominal gout mimicking pelvic abscess. Skeletal Radiol. 2005. 34:229–233.11. Lee CH, Chen YJ, Ueng SW, Hsu RW. Septic arthritis of the ankle joint. Chang Gung Med J. 2000. 23:420–426.12. Yu KH, Luo SF, Liou LB, Wu YJ, Tsai WP, Chen JY, et al. Concomitant septic and gouty arthritis--an analysis of 30 cases. Rheumatology (Oxford). 2003. 42:1062–1066.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tophaceous Gout in the Rotator Cuff with Impingement Syndrome: A Case Report
- Intratendinous Tophaceous Gout Mimicking Cellulitis after Achilles Tendon Repair
- Symptomatic Tophaceous Gout in the Bilateral Patellae
- Tophaceous Gout Involving the Bipartitle Patella: A Case Report
- Two Cases of Chronic Tophaceous Gout in Systemic Lupus Erythematosus
