Analysis of Retinal Nerve Fiber Layer Thickness of Superior Segmental Optic Hypoplasia and Normal-Tension Glaucoma
- Affiliations
-
- 1Department of Ophthalmology, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. kayoungyi@yahoo.co.kr
- 2Department of Ophthalmology, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea.
- 3Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2216671
- DOI: http://doi.org/10.3341/jkos.2013.54.2.331
Abstract
- PURPOSE
To analyze the peripapillary retinal nerve fiber layer (RNFL) in superior segmental optic hypoplasia (SSOH) patients and normal tension glaucoma (NTG) patients with inferior visual field defects using optical coherence tomography (OCT).
METHODS
Ten eyes of 10 patients with SSOH and 10 eyes of 10 patients with NTG were evaluated. The peripapillary RNFL thickness measured by OCT was compared between the 2 groups.
RESULTS
The mean RNFL thickness was not significantly different between SSOH patients (79.60 +/- 12.54 micrometer) and NTG patients (77.10 +/- 8.52 micrometer) (p = 0.089). Among the quadrant parameters, there were no significant differences between the 2 groups (p > 0.05). In a clock-hour analysis, the peripapillary RNFL thickness of the NTG group was significantly thicker than the SSOH group in 12, 1, and 2 o'clock (p = 0.029, 0.007, 0.043, respectively). In contrast, the peripapillary RNFL thickness of the SSOH group was significantly thicker than the SSOH group in 6, and 7 o'clock (p = 0.029, 0.007, respectively).
CONCLUSIONS
Peripapillary RNFL thickness in patients with SSOH was thinner than in those with NTG in the superonasal region, but thicker in the inferotemporal region indicating a different retinal nerve fiber defect pattern between the 2 diseases.
MeSH Terms
Figure
-

Figure 1. A patient with superior segmental optic hypoplasia (SSOH). Representative color disc photograph (A) and retinal nerve fiber layer (RNFL) photograph (B) showing neuroretinal thinning of the superior nasal region with corresponding RNFL defects. (C) Humphrey automated perimetry shows a characteristic inferior visual field defect. (D) Optical coherence tomography (OCT) scan shows the peripapillary RNFL thinning in superior region of the left eye.

Figure 2. Three examples with superior segmental optic hypoplasia (SSOH). Color fundus photograph and retinal nerve fiber layer (RNFL) photograph show optic disc rim thinning in the superior and superonasal segments (A, B, C).
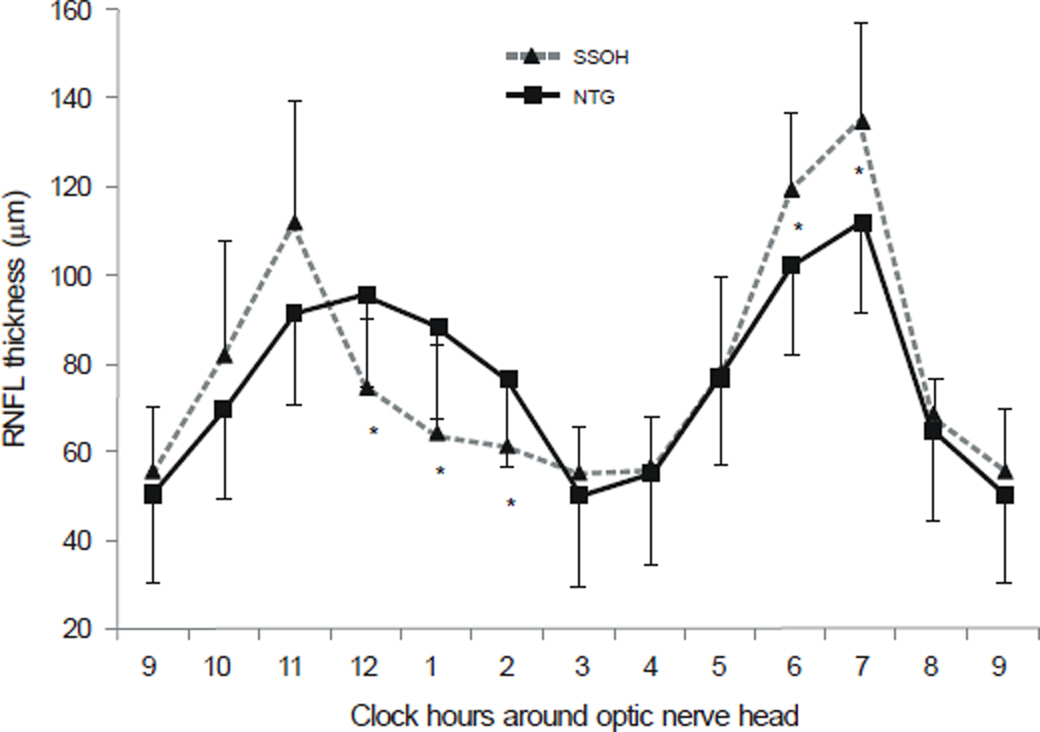
Figure 3. The peripapillary retinal nerve fiber layer (RNFL) thickness assessed by optical coherence tomography is shown for clock hour around the optic nerve head. Solid triangles represent mean RNFL thickness from 10 eyes with superior segmental optic hypoplasia (SSOH) and solid squares represent normal tension glaucoma (NTG) patients. Error bars indicate 1 standard deviation from the mean. Asterisks indicate the clock hours that show significant difference of RNFL thickness between NTG and SSOH patients (p < 0.05).
Reference
-
References
1. Kim RY, Hoyt WF, Lessell S, Narahara MH. Superior segmental optic hypoplasia. A sign of maternal diabetes. Arch Ophthalmol. 1989; 107:1312–5.
Article2. Landau K, Bajka JD, Kirchschläger BM. Topless optic disks in children of mothers with type I diabetes mellitus. Am J Ophthalmol. 1998; 125:605–11.
Article3. Kim TW, Shin KC, Kim DM. Two cases of topless optic disc syndrome. J Korean Ophthalmol Soc. 2000; 41:2291–5.4. Petersen RA, Walton DS. Optic nerve hypoplasia with good visual acuity and visual field defects: a study of children of diabetic mothers. Arch Ophthalmol. 1977; 95:254–8.5. Nelson M, Lessell S, Sadun AA. Optic nerve hypoplasia and maternal diabetes mellitus. Arch Neurol. 1986; 43:20–5.
Article6. Unoki K, Ohba N, Hoyt WF. Optical coherence tomography of superior segmental optic hypoplasia. Br J Ophthalmol. 2002; 86:910–4.
Article7. Yamamoto T, Sato M, Iwase A. Superior segmental optic hypoplasia found in Tajimi Eye Health Care Project participants. Jpn J Ophthalmol. 2004; 48:578–83.
Article8. Hashimoto M, Ohtsuka K, Nakagawa T, Hoyt WF. Topless optic disk syndrome without maternal diabetes mellitus. Am J Ophthalmol. 1999; 128:111–2.
Article9. Purvin VA. Superior segmental optic nerve hypoplasia. J Neuroophthalmol. 2002; 22:116–7.
Article10. Shields MB. Normal-tension glaucoma: is it different from primary open-angle glaucoma? Curr Opin Ophthalmol. 2008; 19:85–8.
Article11. Sommer A, Katz J, Quigley HA, et al. Clinically detectable nerve fiber atrophy precedes the onset of glaucomatous field loss. Arch Ophthalmol. 1991; 109:77–83.
Article12. Lee HJ, Kee C. Optical coherence tomography and Heidelberg retina tomography for superior segmental optic hypoplasia. Br J Ophthalmol. 2009; 93:1468–73.
Article13. Birgbauer E, Cowan CA, Sretavan DW, Henkemeyer M. Kinase independent function of EphB receptors in retinal axon pathfinding to the optic disc from dorsal but not ventral retina. Development. 2000; 127:1231–41.
Article14. Quigley HA, Miller NR, George T. Clinical evaluation of nerve fiber layer atrophy as an indicator of glaucomatous optic nerve damage. Arch Ophthalmol. 1980; 98:1564–71.
Article15. Quigley HA, Addicks EM, Green WR. Optic nerve damage in human glaucoma. III Quantitative correlation of nerve fiber loss and visual field defect in glaucoma, ischemic neuropathy, papilledema, and toxic neuropathy. Arch Ophthalmol. 1982; 100:135–46.
Article16. Sommer A, Miller NR, Pollack I, et al. The nerve fiber layer in the diagnosis of glaucoma. Arch Ophthalmol. 1977; 95:2149–56.
Article17. Choplin NT, Lundy DC, Dreher AW. Differentiating patients with glaucoma from glaucoma suspects and normal subjects by nerve fiber layer assessment with scanning laser polarimetry. Ophthalmology. 1998; 105:2068–76.18. Tuulonen A, Airaksinen PJ. Polarimetry of the retinal nerve fiber layer. Curr Opin Ophthalmol. 1996; 7:34–8.
Article19. Ritch R, Shields MB, Krupin T. The Glaucomas. 2nd Ed. St. Louis, MO: Mosby-Year Book, Inc.;1996. p. 769.20. Woo SW, Choi HW, Kim JS, Lee JH. Correlation between retinal nerve fiber layer thickness and visual field in normal tension glaucoma Patients. J Korean Ophthalmol Soc. 2006; 47:1613–22.21. El Beltagi TA, Bowd C, Boden C, et al. Retinal nerve fiber layer thickness measured with optical coherence tomography is related to visual function in glaucomatous eyes. Ophthalmology. 2003; 110:2185–91.
Article22. Hitchings RA, Anderton SA. A comparative study of visual field defects seen in patients with low-tension glaucoma and chronic simple glaucoma. Br J Ophthalmol. 1983; 67:818–21.
Article23. Caprioli J, Spaeth GL. Comparison of visual field defects in the low-tension glaucomas with those in the high-tension glaucomas. Am J Ophthalmol. 1984; 97:730–7.
Article24. Seo JW, Park IW, Chung YS. Analysis of retinal nerve fiber layer thickness in patients with superior segmental optic hypoplasia. J Korean Ophthalmol Soc. 2009; 50:139–44.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Evaluation of Unilateral Open-Angle Glaucoma: A Two-Year Follow-Up Study
- Correlation Between Disc Size and Retinal Nerve Fiber Layer Thickness in Normal Tension Glaucoma
- Analysis of Retinal Nerve Fiber Layer Thickness in Patients With Superior Segmental Optic Hypoplasia
- Differentiating Patients with Glaucoma from Glaucoma Suspects by Retinal Nerve Fiber Layer Assessment Using Nerve Fiber Analyzer
- Reproducibility of Retinal Nerve Fiber Layer Thickness Evaluation by Nerve Fiber Analyzer
