J Korean Ophthalmol Soc.
2013 Feb;54(2):324-330. 10.3341/jkos.2013.54.2.324.
The Clinical Characteristics of V-Pattern Exotropia Without Inferior Oblique Muscle Overaction
- Affiliations
-
- 1Department of Ophthalmology, Chungbuk National University School of Medicine, Cheongju, Korea. mychoi@chungbuk.ac.kr
- KMID: 2216670
- DOI: http://doi.org/10.3341/jkos.2013.54.2.324
Abstract
- PURPOSE
To compare the surgical outcome between V-pattern intermittent exotropia without inferior oblique overaction and comitant intermittent exotropia.
METHODS
The authors of the present study investigated 15 patients (V-pattern group) who had standard horizontal surgery with half-tendon width vertical transposition and 36 patients (Comitant group) with unilateral rectus muscle recession/resection. Preoperative visual acuity, presence of amblyopia, abnormal head posture, stereoacuity, amount of exotropia, and duration of postoperative diplopia were recorded. Surgical success was defined as final alignment of orthophoria or less than 10 PD orthophoria.
RESULTS
The frequency of good stereoacuity with 80 sec of stereoacuity or more was higher in the V-pattern group (73.3%) than in the Comitant group (33.3%) (Fisher's exact test, p = 0.01). One case of V-pattern showed consecutive esotropia for 1 year postoperatively. Exotropia recurred in 2 patients in the V-pattern group (13.3%), and in 4 patients in the Comitant group (11.1%) 1 year postoperatively. Surgical success rates were statistically significant higher in the V-pattern group (86.7%) as compared to the Comitant group (58.3%) on final follow-up (Fisher's exact test, p = 0.04).
CONCLUSIONS
V-pattern exotropia patients without inferior oblique overaction who had standard horizontal surgery with half-tendon width vertical transposition showed a lower recurrence rate of exotropia than patients with comitant intermittent exotropia.
MeSH Terms
Figure
-
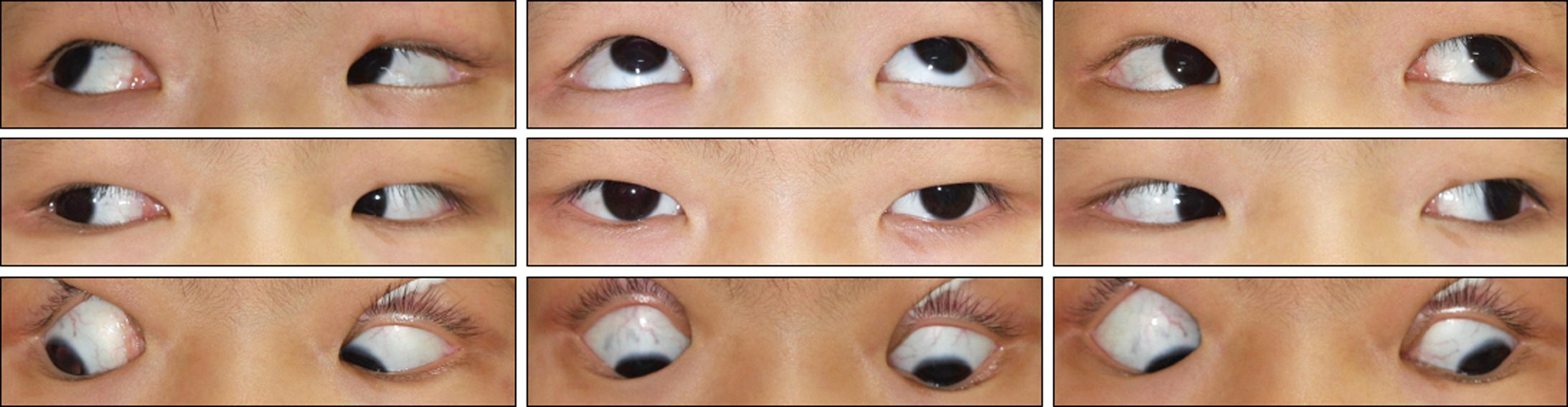
Figure 1. 9-Gaze photograph shows V-pattern exotropia without overacting inferior oblique muscles. This case shows exotropia in primary gaze, decrease of exotropic deviation in downgaze and increase of exotropic deviation in upgaze. Inferior oblique muscles are not overacting when the patient fixates to the right, left, right and up, and left and up directions.
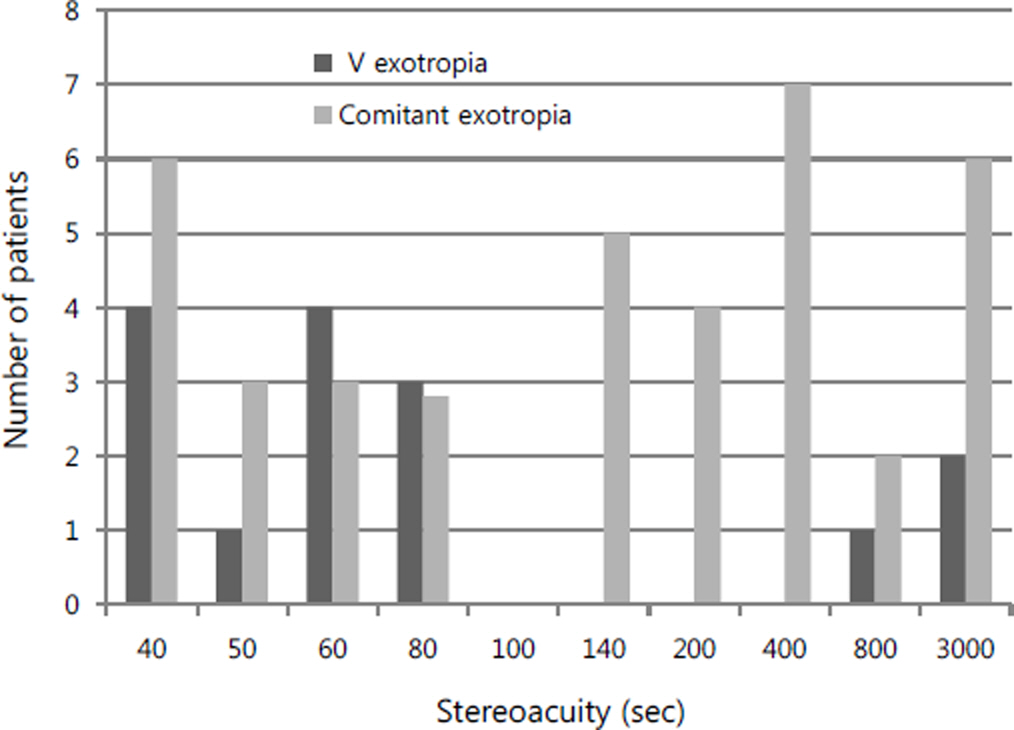
Figure 2. Distribution of stereopsis between the 2 treatment groups.

Figure 3. The change of postoperative deviation angle during follow-up. - means esotropia, + means exotropia. There was no statistically significance in postoperative deviation angle between the 2 treatment groups during each follow-up period (Mann-W hitney test, final follow-up p = 0.17).
Reference
-
References
1. Raab EL, Parks MM. Recession of the lateral recti. Early and late postoperative alignments. Arch Ophthalmol. 1969; 82:203–8.
Article2. Lee S, Lee YC. Relationship between motor alignment at postoperative day 1 and at year 1 after symmetric and asymmetric surgery in intermittent exotropia. Jpn J Ophthalmol. 2001; 45:167–71.
Article3. Eino D, Kraft SP. Postoperative drifts after adjustable-suture strabismus surgery. Can J Ophthalmol. 1997; 32:163–9.4. Albert DG. Personal communication. In: Parks MM. Annual review Strabismus. Arch Ophthalmol. 1957; 58:152.5. Pineles SL, Rosenbaum AL, Demer JL. Decreased postoperative drift in intermittent exotropia associated with A and V patterns. J AAPOS. 2009; 13:127–31.
Article6. Lee SY. Comparison of distance and near stereoacuity in normal and intermittent exotropic children. J Korean Ophthalmol Soc. 2001; 42:624–9.7. Rosenbaum AL. Clinical Strabismus Management. 1st ed. Philadelphia: Saunders;1999. p. 16–7.8. Wright KW. Color Atlas of Ophthalmic Surgery: Strabismus. Philadelphia: JB Lippincott Co;1991. p. 241.9. Urist MJ. The etiology of the so-called A and V syndromes. Am J Ophthalmol. 1958; 46:835–44.
Article10. Brown HW. Symposium; strabismus; vertical deviations. Trans Am Acad Ophthalmol Otolaryngol. 1953; 57:157–62.11. Knapp P. Vertically incomitant Horizontal Strabismus: The So-called “A” and “V” Syndromes. Trans Am Ophthalmol Soc. 1959; 57:666–99.12. Yu XP, Mai GH, Yu HY, et al. [Clinical features of V patterns strabismus and its long-term effect of surgical treatment]. Zhonghua Yan Ke Za Zhi. 2005; 41:585–9.13. Chang WS, Kim SY. Clinical study of A-V pattern strabismus in Korea. J Korean Ophthalmol Soc. 2008; 49:1974–80.
Article14. Postic G. Etiopathogenie des syndrome A et V. Bull Mem Soc Fr Ophthalmol. 1965; 78:240–52.15. Metz HS, Schwartz L. The treatment of A and V patterns by monocular surgery. Arch Ophthalmol. 1977; 95:251–3.
Article16. Scott WE, Drummond GT, Keech RV. Vertical offsets of horizontal recti muscles in the management of A and V pattern strabismus. Aust N Z J Ophthalmol. 1989; 17:281–8.
Article17. Oya Y, Yagasaki T, Maeda M, et al. Effects of vertical offsets of the horizontal rectus muscles in V-pattern exotropia without oblique dysfunction. J AAPOS. 2009; 13:575–7.
Article18. Heo NH, Paik HJ. The relationship between binocular function and the surgical outcome of intermittent exotropia. J Korean Ophthalmol Soc. 2001; 42:1588–93.19. Caldeira JA. Some clinical characteristics of V-pattern exotropia and surgical outcome after bilateral recession of the inferior oblique muscle: a retrospective study of 22 consecutive patients and a comparison with V-pattern esotropia. Binocul Vis Strabismus Q. 2004; 19:139–50.20. Lee SY, Rosenbaum AL. Surgical results of patients with A-pattern horizontal strabismus. J AAPOS. 2003; 7:251–5.
Article21. Pollard ZF. Superior oblique tenectomy in a pattern strabismus. Ann Ophthalmol. 1978; 10:211–5.22. Shuey TF Jr, Parks MM, Friendly DS. Results of combined surgery on the superior oblique and horizontal rectus muscles for A-pattern horizontal strabismus. J Pediatr Ophthalmol Strabismus. 1992; 29:199–201.
Article23. Hatt SR, Mohney BG, Leske DA, Holmes JM. Variability of stereoacuity in intermittent exotropia. Am J Ophthalmol. 2008; 145:556–61.
Article24. Miller M, Folk E. Strabismus associated with craniofacial anomalies. Am Orthopt J. 1975; 25:27–37.
Article25. Demer JL, Clarks RA, Miller JM. Heterotopy of extraocular muscle pulleys causes incomitant strabismus: In Lennerstrand G, ed. Advances in Strabismology. Proceedings of the Eighth Meeting of the International Strabismological Association, Maastricht. Sep. 10-12. 1998. Buren, The Netherlands: Aeolus Press;1999. p. 91.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Secondary Superior Oblique Overaction after Inferior Oblique Muscle Myectomy in a Patient Misdiagnosed with Inferior Oblique Muscle Overaction
- A Study on the Anatomical Position of the Inferior Oblique Muscle Insertion in Primary Inferior Oblique Overaction
- The Effect of Anteriorization of The Inferior Oblique Muscle in +3 or +4 Inferior Oblique Overaction
- The Effect of Anterior Transposition with J-Deformity for Overaction of the Inferior Oblique Muscle
- The Effect of Inferior Oblique Muscle Transposition in Primary and Secondary Inferior Oblique Muscle Overaction
