J Korean Ophthalmol Soc.
2012 Sep;53(9):1291-1295. 10.3341/jkos.2012.53.9.1291.
Visual and Surgical Outcomes of Lamellar Macular Hole
- Affiliations
-
- 1Sungmo Eye Hospital, Busan, Korea. heesyoon@dreamwiz.com
- KMID: 2216082
- DOI: http://doi.org/10.3341/jkos.2012.53.9.1291
Abstract
- PURPOSE
To investigate the visual and anatomical results of surgical treatment for symptomatic lamellar macular hole.
METHODS
Ten eyes of ten patients with decreased visual acuity and lamellar macular hole were diagnosed using optical coherence tomography (OCT). Pars plana vitrectomy, epiretinal membrane removal, internal limiting membrane peeling, and gas tamponade (5 eyes) were performed for the treatment of lamellar hole. The resolution of the lamellar hole was assessed in relation to each OCT image at baseline.
RESULTS
The mean postoperative follow-up duration was 7.5 months, and best corrected visual acuity improved from log MAR 0.67 +/- 0.38 to log MAR 0.30 +/- 0.28. Central foveal thickness decreased from 441 +/- 184 microm to 291 +/- 64 microm. The OCT of all eyes demonstrated improvement in macular contour. However, retinal detachment in one eye occurred at two months after the operation and was reattached with gas tamponade and photocoagulation.
CONCLUSIONS
Vitrectomy, epiretinal membrane removal and internal limiting membrane peeling showed benefit in the treatment of symptomatic lamellar macular hole. However, large and prospective studies are necessary regarding the surgical indication, time and procedure for lamella macular hole.
Keyword
MeSH Terms
Figure
-
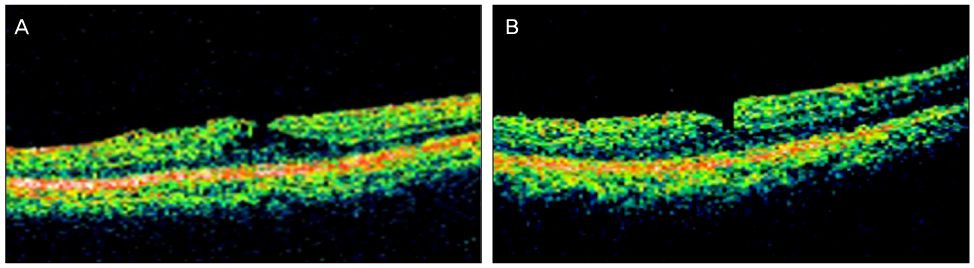
Figure 1 (A) Preoperative OCT images with visual acuity log MAR 0.40 and foveal thickness 357 µm. This image fulfills the criteria for OCT diagnosis of lamellar hole: (1) irregular foveal contour; (2) dehiscence in the inner fovea; (3) separation of the inner from the outer foveal retinal layers, leading to an intraretinal split; (4) absence of a full-thickness foveal defect. (B) OCT at 2 months after operation with visual acuity log MAR 0.22 and foveal thickness 331 µm.
Cited by 1 articles
-
The Evaluation of Prognostic Factors after Vitrectomy for Lamellar Macular Hole Using Optical Coherence Tomography
Sang Won Kim, Hye Min Jeon, Dong Seob Ahn, Hee Seong Yoon
J Korean Ophthalmol Soc. 2014;55(12):1853-1859. doi: 10.3341/jkos.2014.55.12.1853.
Reference
-
1. Gass JD. Lamellar macular hole: a complication of cystoid macular edema after cataract extraction: a clinicopathologic case report. Trans Am Ophthalmol Soc. 1975. 73:231–250.2. Haouchine B, Massin P, Tadayoni R, et al. Diagnosis of macular pseudoholes and lamellar macular holes by optical coherence tomography. Am J Ophthalmol. 2004. 138:732–739.3. Haouchine B, Massin P, Gaudric A. Foveal pseudocyst as the first step in macular hole formation: a prospective study by optical coherence tomography. Ophthalmology. 2001. 108:15–22.4. Witkin AJ, Ko TH, Fujimoto JG, et al. Redefining lamellar holes and the vitreomacular interface: an ultrahigh-resolution optical coherence tomography study. Ophthalmology. 2006. 113:388–397.5. Tanner V, Chauhan DS, Jackson TL, Williamson TH. Optical coherence tomography of the vitreoretinal interface in macular hole formation. Br J Ophthalmol. 2001. 85:1092–1097.6. Androudi S, Stangos A, Brazitikos PD. Lamellar macular holes: tomographic features and surgical outcome. Am J Ophthalmol. 2009. 148:420–426.7. Kelly NE, Wendel RT. Vitreous surgery for idiopathic macular holes. Results of a pilot study. Arch Ophthalmol. 1991. 109:654–659.8. Garretson BR, Pollack JS, Ruby AJ, et al. Vitrectomy for a symptomatic lamellar macular hole. Ophthalmology. 2008. 115:884–886.9. Chen J, Lee L. Clinical applications and new developments of optical coherence tomography: an evidence-based review. Clin Exp Optom. 2007. 90:317–335.10. Witkin AJ, Castro LC, Reichel E, et al. Anatomic and visual outcomes of vitrectomy for lamellar macular holes. Ophthalmic Surg Lasers Imaging. 2010. 41:418–424.11. Michalewska Z, Michalewski J, Odrobina D, et al. Surgical treatment of lamellar macular holes. Graefes Arch Clin Exp Ophthalmol. 2010. 248:1395–1400.12. Cho WB, Shin HJ, Moon JW, Kim HC. Four cases of pars plana vitrectomy for treatment of symptomatic lamellar macular holes. J Korean Ophthalmol Soc. 2009. 50:1427–1431.13. Altaweel M, Ip M. Macular hole: improved understanding of pathogenesis, staging, and management based on optical coherence tomography. Semin Ophthalmol. 2003. 18:58–66.14. Leung CK, Cheung CY, Weinreb RN, et al. Comparison of macular thickness measurements between time domain and spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2008. 49:4893–4897.15. Kakinoki M, Sawada O, Sawada T, et al. Comparison of macular thickness between Cirrus HD-OCT and Stratus OCT. Ophthalmic Surg Lasers Imaging. 2009. 40:135–140.16. Chen JC, Lee LR. Clinical spectrum of lamellar macular defects including pseudoholes and pseudocysts defined by optical coherence tomography. Br J Ophthalmol. 2008. 92:1342–1346.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Vitrectomy on the Treatment of a Lamellar Macular Hole in Highly Myopic Patients
- The Evaluation of Prognostic Factors after Vitrectomy for Lamellar Macular Hole Using Optical Coherence Tomography
- Postoperative Changes in Vessel Density according to Macular Hole and Macular Pseudohole Subtypes
- Long-Term Visual Outcomes and Prognostic Factors for Successful Idiopathic Macular Hole
- Epiretinal Proliferation Associated with Lamellar Hole or Macular Hole: Origin and Surgical Prognosis
