Efficacy of the Sutureless Amniotic Membrane Patch for the Treatment of Ocular Surface Disorders
- Affiliations
-
- 1Department of Ophthalmology, Daegu Fatima Hospital, Daegu, Korea. djoph2540@yahoo.co.kr
- KMID: 2215242
- DOI: http://doi.org/10.3341/jkos.2012.53.1.27
Abstract
- PURPOSE
To evaluate the efficacy of the sutureless amniotic membrane (AM) patch for the treatment of ocular surface disorders.
METHODS
A sutureless AM patch using a silicone ring was utilized to treat neurotrophic ulcer, persistent epithelial defect (PED), Shield ulcer, chemical injury and Stevens-Johnson syndrome. Primary outcome was the time to complete corneal and conjunctival epithelialization. Secondary outcome was the number of repeated insertions and complications of the inserted ring.
RESULTS
Neurotrophic ulcer was observed in 4 eyes, PED in 2 eyes, Shield ulcer in 1 eye, chemical injury in 4 eyes and Stevens-Johnson syndrome in 4 eyes. The mean (SD) time to complete epithelialization was 13 (7.2) days (6-20 days) in neurotrophic ulcer, 17.5 (7.7) days (12-23) in PED, 5 days in Shield ulcer, 10.6 (6.6) days (3-15) in chemical injury and 13.5 (0.7) days (13-14) in Stevens-Johnson syndrome. There were no protrusion or mechanical trauma of the inserted ring. In 1 case of neurotrophic ulcer and 1 refractory case of chemical injury, repeated insertion was performed due to incomplete healing after dissolution of the AM. In 2 eyes with Stevens-Johnson syndrome, repeated insertion was necessary with heavy accumulation of inflammatory debris on the AM. No symblepharon or fornix contracture was found in chemical injury or Stevens-Johnson syndrome patients.
CONCLUSIONS
The sutureless AM patch using a silicone ring was shown to be effective and safe for the treatment of ocular surface disorders. The patch can help surgeons avoid suture-related trauma to the ocular surface during the acute inflammatory period.
Keyword
Figure
-

Figure 1 Surgical amniotic membrane transplantation for Stevens-Johnson syndrome requires lots of sutures (A) and bolster suture (B) that may irritate the ocular surface even worse.

Figure 2 The structure of the 2 types of amniotic membrane fixation silicone ring: round (A) and oval (B).

Figure 3 The selected silicone ring (either round or oval) is placed on the amniotic membrane (AM) (A) and wrapped up with the AM carefully peeled off the nitrocellulose paper from one end to the other (B, C, D, E). The AM is fixed on the silicone ring with 10-0 nylon and the completed AM fixation silicone ring (F) is ready to be placed in the patient's eye right away.
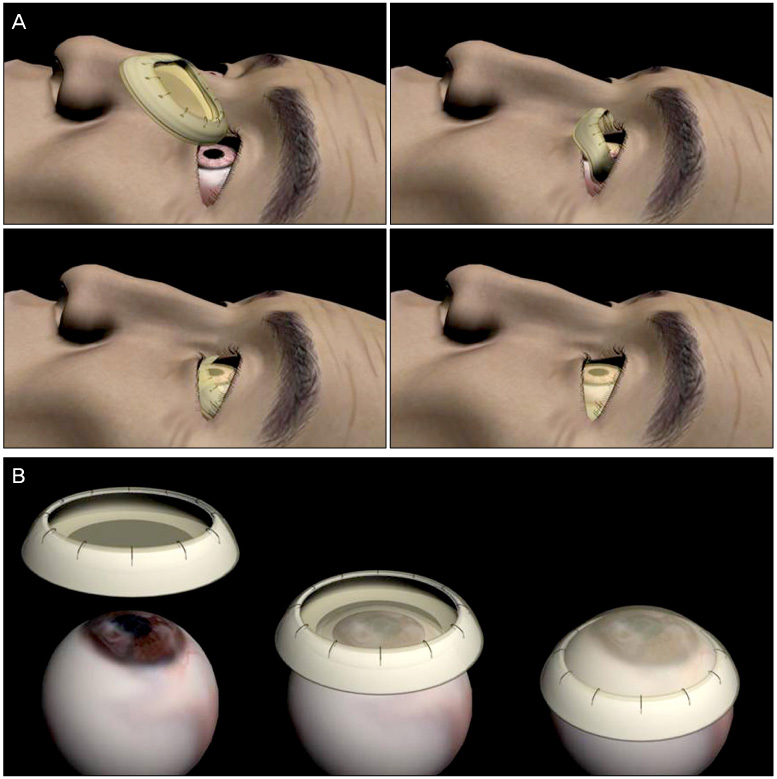
Figure 4 Silicone ring fixed with amniotic membrane patch is inserted deep into the fornix (A). Its various sizes and flexibility makes it easy to fit in small eyes as well. The amniotic membrane is expanded and closely adhered to the ocular surface due to its elasticity (B).
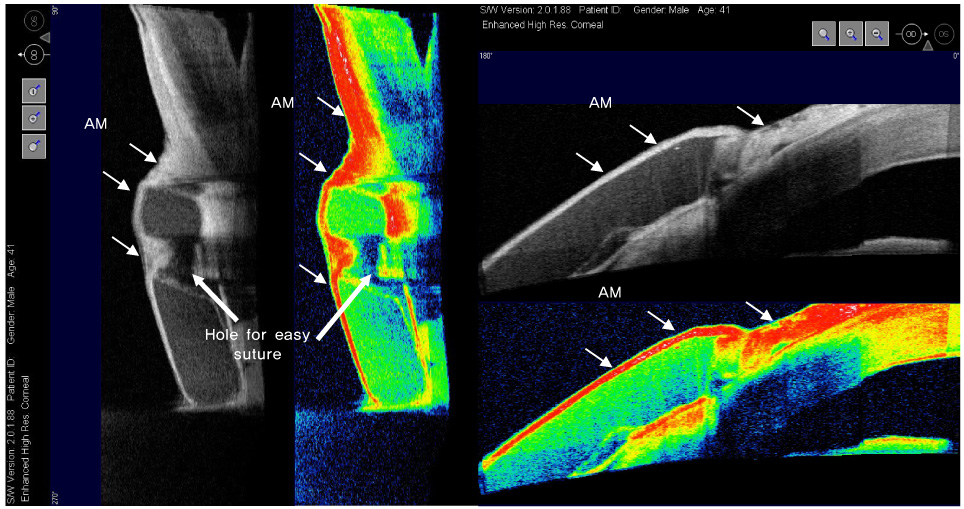
Figure 5 The amniotic membrane fixation silicone ring is well placed in the fornix and the amniotic membrane (AM, white short arrows) is adhered closely to the ocular surface (patient 8) confirmed by the anterior segment optical coherence tomography (Visante OCT; Carl Zeiss Meditec, Dublin, CA). Notice the hole on the silicone ring for easy suture on fixing the AM on the ring.
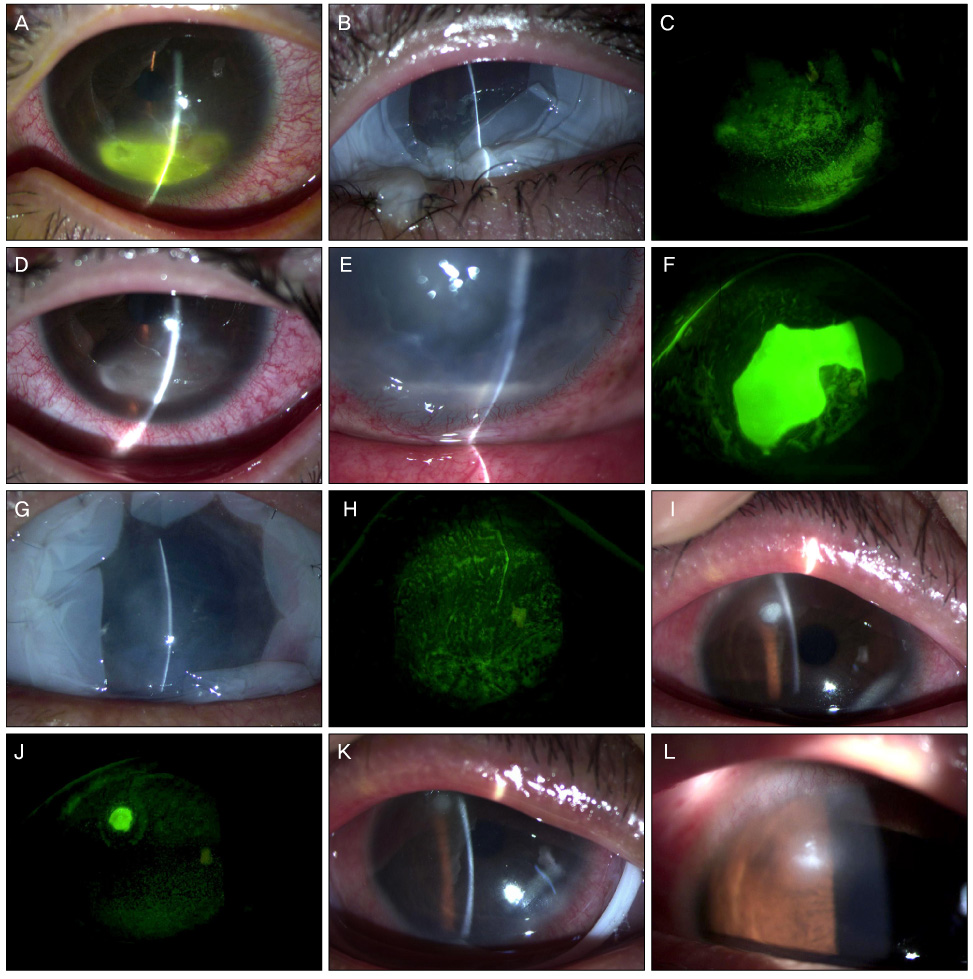
Figure 6 Outcomes of non-surgical amniotic membrane patch using round silicone ring. Patient 3, neurotrophic ulcer patient with corneal epithelial defect and opacity (A). Round AM ring was inserted (B) and additional AM ring was exchanged due to dissolution of AM before complete epithelialization. Epithelial defect was healed 19 days after the first insertion (C, D). Patient 5, PED patient (previous visual loss due to diabetic retinopathy) with corneal epithelial defect (E) (with fluorescein staining [F]) showed marked reepithelialization after insertion of AM ring (G) and closure of epithelial defect after 12 days (H). Patient 7, Shield ulcer patient with corneal epithelial defect (I, J). Round AM ring was inserted (K) and epithelium was healed in 5 days (L).
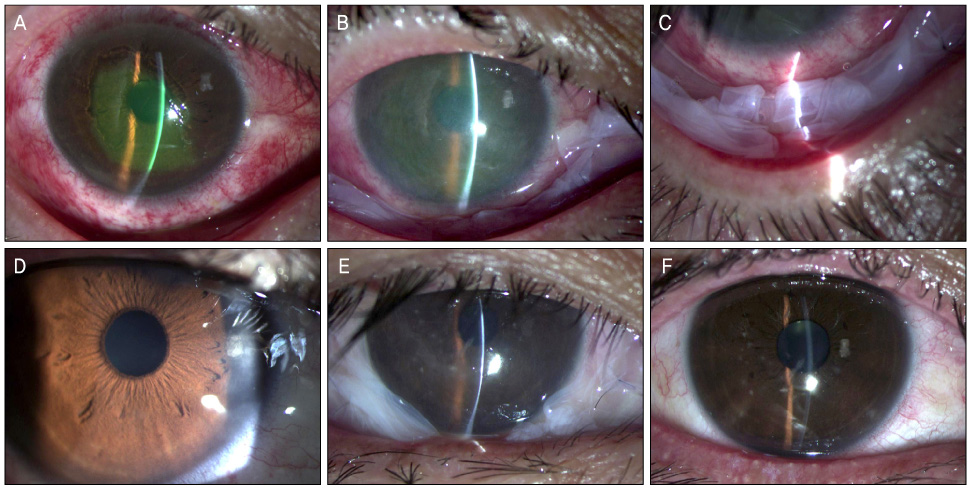
Figure 7 Outcomes of non-surgical amniotic membrane patch using oval silicone ring. Patient 9, chemical injury patient with extensive corneal and conjunctival epithelial defects (A) showed healing of the defects after insertion (B, C) and smooth and stable ocular surface 3 days later (D). Patient 12, Stevens-Johnson syndrome patient with surface defects and corneal opacity showed improvement 13 days after insertion (E) and a stable surface with faint corneal opacity (F).

Figure 8 Comparison of ProKera® (left) and silicone ring for amniotic membrane (AM) fixation (right). AM ring is entirely covered with amniotic membrane that can adhere to the entire ocular surface and its flexibility reduces discomfort.
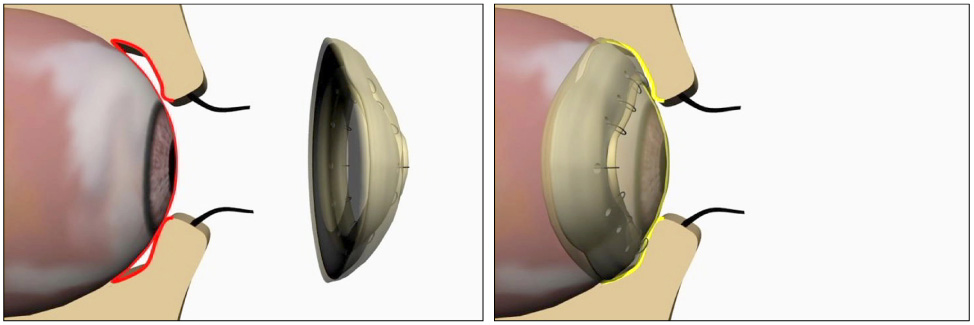
Figure 9 The oval ring can adhere to not only the bulbar conjunctiva but the palpebral conjunctiva that maintains the fornix and prevents symblepharon.
Reference
-
1. de Rötth A. Plastic repair of conjunctival defects with fetal membranes. Arch Ophthalmol. 1940. 23:522–525.2. Kim JC, Tseng SC. Transplantation of preserved human amniotic membrane for surface reconstruction in severely damaged rabbit corneas. Cornea. 1995. 14:473–484.3. Tseng SC, Prabhasawat P, Lee SH. Amniotic membrane transplantation for conjunctival surface reconstruction. Am J Ophthalmol. 1997. 124:765–774.4. Tsubota K, Satake Y, Ohyama M, et al. Surgical reconstruction of the ocular surface in advanced ocular cicatricial pemphigoid and Stevens-Johnson syndrome. Am J Ophthalmol. 1996. 122:38–52.5. Pires RT, Tseng SC, Prabhasawat P, et al. Amniotic membrane transplantation for symptomatic bullous keratopathy. Arch Ophthalmol. 1999. 117:1291–1297.6. Tseng SC, Prabhasawat P, Barton K, et al. Amniotic membrane transplantation with or without limbal allografts for corneal surface reconstruction in patients with limbal stem cell deficiency. Arch Ophthalmol. 1998. 116:431–441.7. Chun DH, Jeon SL, Lee JY, Choi TH. The effect of amniotic membrane transplantation on corneal epithelial cell proliferation. J Korean Ophthalmol Soc. 2002. 43:1746–1757.8. Shin KS, Chung IY, Seo SW. The effect of amniotic membrane transplantation for corneal ulcer and ocular surface diseases. J Korean Ophthalmol Soc. 2003. 44:1305–1310.9. Lee SH, Tseng SC. Amniotic membrane transplantation for persistent epithelial defects with ulceration. Am J Ophthalmol. 1997. 123:303–312.10. Kruse FE, Rohrschneider K, Völcker HE. Multilayer amniotic membrane transplantation for reconstruction of deep corneal ulcers. Ophthalmology. 1999. 106:1504–1510.11. Roper-Hall MJ. Thermal and chemical burns. Trans Ophthalmol Soc UK. 1965. 85:631–653.12. Kheirkhah A, Johnson DA, Paranipe DR, et al. Temporary sutureless amniotic membrane patch for acute alkaline burns. Arch Ophthalmol. 2008. 126:1059–1066.13. Pachigolla G, Prasher P, Di Pascuale MA, et al. Evaluation of the role of ProKera in the management of ocular surface and orbital disorders. Eye Contact Lens. 2009. 35:172–175.14. Sheha H, Liang L, Li J, Tseng SC. Sutureless amniotic membrane transplantation for severe bacterial keratitis. Cornea. 2009. 28:1118–1123.15. Shammas MC, Lai EC, Sarkar JS, et al. Management of acute Stevens-Johnson syndrome and toxic epidermal necrolysis utilizing amniotic membrane and topical corticosteroids. Am J Ophthalmol. 2010. 149:203–213.16. Shay E, Khadem JJ, Tseng SC. Efficacy and limitation of sutureless amniotic membrane transplantation for acute toxic epidermal necrolysis. Cornea. 2010. 29:359–361.17. Uçakhan OO, Köklü G, Firat E. Nonpreserved human amniotic membrane transplantation in acute and chronic chemical eye injuries. Cornea. 2002. 21:169–172.18. Kobayashi A, Shirao Y, Yoshita T, et al. Temporary amniotic membrane patching for acute chemical burns. Eye (Lond). 2003. 17:149–158.19. Arora R, Mehta D, Jain V. Amniotic membrane transplantation in acute chemical burns. Eye (Lond). 2005. 19:273–278.20. Tamhane A, Vajpayee RB, Biswas NR, et al. Evaluation of amniotic membrane transplantation as an adjunct to medical therapy as compared with medical therapy alone in acute ocular burns. Ophthalmology. 2005. 112:1963–1969.21. Prabhasawat P, Tesavibul N, Prakairungthong N, Booranapong W. Efficacy of amniotic membrane patching for acute chemical and thermal ocular burns. J Med Assoc Thai. 2007. 90:319–326.22. López-García JS, Rivas Jara L, García-Lozano I, Murube J. Histopathologic limbus evolution after alkaline burns. Cornea. 2007. 26:1043–1048.23. Joseph A, Dua HS, King AJ. Failure of amniotic membrane transplantation in the treatment of acute ocular burns. Br J Ophthalmol. 2001. 85:1065–1069.24. Mackie IA. Role of the corneal nerves in destructive disease of the cornea. Trans Ophthalmol Soc U K. 1978. 98:343–347.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Applications and Complications of Contact Lens Type Amniotic Membrane
- New Strategy of Ocular Surface Disease: Ocular Surface Reconstruction Using Amniotic Membrane and Limbal Stem Cell Transplantation
- Clinical Benefits of Amniotic Membrane Contact Lens
- Ocular Surface Reconstruction with Amniotic Membrane Transplantation in Pterygium
- A Novel Application of Amniotic Membrane in Patients with Bullous Keratopathy
