J Korean Surg Soc.
2012 Oct;83(4):196-202. 10.4174/jkss.2012.83.4.196.
Observational study of central metastases following thyroid lobectomy without a completion thyroidectomy for papillary carcinoma
- Affiliations
-
- 1Department of Surgery, Chonnam National University Medical School, Gwangju, Korea. this0100@gmail.com
- 2Department of Pathology, Chonnam National University Medical School, Gwangju, Korea.
- 3Department of Internal Medicine, Chonnam National University Medical School, Gwangju, Korea.
- KMID: 2212303
- DOI: http://doi.org/10.4174/jkss.2012.83.4.196
Abstract
- PURPOSE
There are no guidelines for the optimal timing of the decision of when to perform completion thyroidectomy, and controversy exists regarding how the timing of completion thyroidectomy impacts survival patterns. We investigated the legitimacy of an observational strategy in central node metastasis after thyroid lobectomy for papillary thyroid cancer (PTC).
METHODS
We retrospectively evaluated 522 consecutive patients who underwent thyroid lobectomy. Of the 69 patients with central metastasis, 61 patients (88.4%) were included in an observational study under cautious evaluation with informed consent by the patients, and compared with an observation arm of 180 postlobectomy N0 (node negative proven) patients.
RESULTS
Of the 522 patients, six (1.1%) thyroid, five (0.9%) central, and two (0.4%) lateral recurrences were observed. Lateral recurrences occurred in the immediate completion N0 and Nx groups but not in the N1a observation arms. There were two (3.3%) central recurrences without thyroid or lateral recurrence on the observation arm of N1a observation patients. But two (1.1%) thyroid and three (1.7%) central recurrences were on the observation arm of N0 patients. In Kaplan-Meier survival curves for central or lateral recurrences between observation arms for the N1a and N0 groups, no significant difference was found between the N1a and N0 observation arms (P = 0.365).
CONCLUSION
The timing of when to perform completion thyroidectomy in central metastases-proven patients after lobectomy for PTC should be based on the patient's risk category.
MeSH Terms
Figure
-
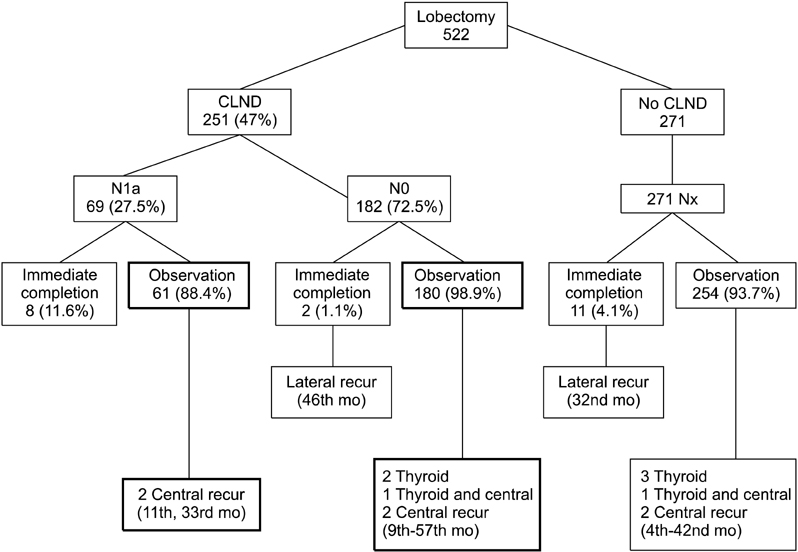
Fig. 1 Follow-up of 522 patients underwent lobectomy due to papillary thyroid cancer. CLND, central lymph node dissection.
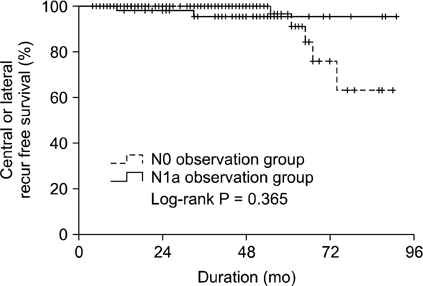
Fig. 2 Kaplan-Meier survival curves for central or lateral recurrences according to observation arm of N1a versus N0 groups (P = 0.365, log-rank test).
Cited by 1 articles
-
A Clinical Analysis of Endoscopic Thyroidectomy via Bilateral Axillobreast Approach: A 5-year Experience
Yun Chul Park, Young Jae Ryu, Jin Seong Cho, Jung Han Yoon, Min Ho Park
Korean J Endocr Surg. 2015;15(2):41-46. doi: 10.16956/kjes.2015.15.2.41.
Reference
-
1. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer. Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009. 19:1167–1214.2. Sherman SI, Angelos P, Ball DW, Byrd D, Clark OH, Daniels GH, et al. Thyroid carcinoma. J Natl Compr Canc Netw. 2007. 5:568–621.3. Shaha AR. Extent of surgery for papillary thyroid carcinoma: the debate continues: comment on "surgery for papillary thyroid carcinoma". Arch Otolaryngol Head Neck Surg. 2010. 136:1061–1063.4. Cho JS, Shin SH, Song YJ, Kim HK, Park MH, Yoon JH, et al. Is it possible to predict hypothyroidism after thyroid lobectomy through thyrotropin, thyroglobulin, anti-thyroglobulin, and anti-microsomal antibody? J Korean Surg Soc. 2011. 81:380–386.5. Choe JH, Kim SW, Chung KW, Park KS, Han W, Noh DY, et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World J Surg. 2007. 31:601–606.6. Mendelsohn AH, Elashoff DA, Abemayor E, St John MA. Surgery for papillary thyroid carcinoma: is lobectomy enough? Arch Otolaryngol Head Neck Surg. 2010. 136:1055–1061.7. Hay ID, Bergstralh EJ, Goellner JR, Ebersold JR, Grant CS. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery. 1993. 114:1050–1057.8. Hay ID. Papillary thyroid carcinoma. Endocrinol Metab Clin North Am. 1990. 19:545–576.9. DeGroot LJ, Kaplan EL, McCormick M, Straus FH. Natural history, treatment, and course of papillary thyroid carcinoma. J Clin Endocrinol Metab. 1990. 71:414–424.10. Sherman SI. The risks of thyroidectomy: words of caution for referring physicians. J Gen Intern Med. 1998. 13:60–61.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Thyroid Lobectomy as an Initial Treatment Option on 1-4 cm Papillary Cancer
- Occult Papillary Thyroid Carcinoma Presenting as a Metastatic Pleural Effusion
- Concurrent Papillary and Medullary Carcinoma of the Thyroid Gland
- The Clinicopathological Features and Postoperative Complications of Completion Thyroidectomy for Recurrent Papillary Thyroid Carcinoma
- Is Completion Thyroidectomy Necessary in Patients with Papillary Thyroid Carcinoma who Underwent Lobectomy?
