J Korean Surg Soc.
2011 Sep;81(3):169-175. 10.4174/jkss.2011.81.3.169.
Long-term results in the treatment of fistula-in-ano with fibrin glue: a prospective study
- Affiliations
-
- 1Department of General Surgery, Gaziantep University Faculty of Medicine, Gaziantep, Turkey. gokturkm2@gmail.com
- KMID: 2212194
- DOI: http://doi.org/10.4174/jkss.2011.81.3.169
Abstract
- PURPOSE
This prospective study was done to analyze the efficacy of commercial fibrin glue application in the healing of patients with fistulas-in-ano from a long-term (mean 4.5 years) research period.
METHODS
This clinical trial of forty-six patients was performed during the period from January 2004 to February 2005. Thirty-nine men and seven women were treated for a fistula-in-ano with a commercial fibrin glue application. In the operating room, the patients underwent an anorectal examination under spinal anesthesia. The external and internal fistula tract openings were then identified. The fistula tract was curetted. Fibrin glue was injected into the external fistula opening until the fibrin glue could be seen coming from the internal opening.
RESULTS
The overall initial success rate was 86.95% (40/46). Recurrence rate was 41.30% (19/46). Two patients underwent a re-application with fibrin glue and the fistulas of these patients closed. The total recurrence rate was 36.95% (17/46). The long-term overall success rate was 63.04% (29/46).
CONCLUSION
Fibrin glue application was thus found to be an easy, safe, acceptable, successful alternative treatment in the management of fistulas-in-ano. Choosing the patient correctly is very important because long (more than 4 cm) and non-ramificate fistula tracts usually close with commercial fibrin glue.
Keyword
MeSH Terms
Figure
-
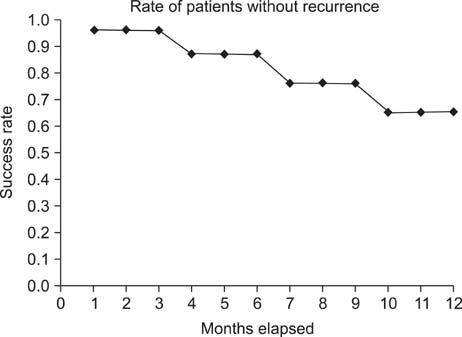
Fig. 1 Kaplan Meier curve for recurrence cases
Reference
-
1. Sentovich SM. Fibrin glue for all anal fistulas. J Gastrointest Surg. 2001. 5:158–161.2. Lunniss PJ, Kamm MA, Phillips RK. Factors affecting continence after surgery for anal fistula. Br J Surg. 1994. 81:1382–1385.3. Maralcan G, Başkonuş I, Aybasti N, Gökalp A. The use of fibrin glue in the treatment of fistula-in-ano: a prospective study. Surg Today. 2006. 36:166–170.4. Hammond TM, Grahn MF, Lunniss PJ. Fibrin glue in the management of anal fistulae. Colorectal Dis. 2004. 6:308–319.5. Kim HH, Park EK, Seoung JS, Hur YH, Koh YS, Kim JC, et al. Liver resection for hepatocellular carcinoma: case-matched analysis of laparoscopic versus open resection. J Korean Surg Soc. 2011. 80:412–419.6. Venkatesh KS, Ramanujam P. Fibrin glue application in the treatment of recurrent anorectal fistulas. Dis Colon Rectum. 1999. 42:1136–1139.7. Khafagy W, Zedan W, Setiet A, El-Awady S, El-Shobaky MT. Autologous fibrin glue in treatment of fistula in ano. Coloproctology. 2001. 23:17–21.8. Levine RJ, editor. World Medical Association Declaration of Helsinki Recommendations guiding medical doctors in biomedical research involving human subjects. Ethics and regulation of clinical research. 1981. Baltimore: Urban and Schwarzenberg;287–289.9. Hedelin H, Nilson AE, Teger-Nilsson AC, Thorsen G. Fibrin occlusion of fistulas postoperatively. Surg Gynecol Obstet. 1982. 154:366–368.10. Kirkegaard P, Madsen PV. Perineal sinus after removal of the rectum. Occlusion with fibrin adhesive. Am J Surg. 1983. 145:791–794.11. Abel ME, Chiu YS, Russell TR, Volpe PA. Autologous fibrin glue in the treatment of rectovaginal and complex fistulas. Dis Colon Rectum. 1993. 36:447–449.12. Lange V, Meyer G, Wenk H, Schildberg FW. Fistuloscopy: an adjuvant technique for sealing gastrointestinal fistulae. Surg Endosc. 1990. 4:212–216.13. Hjortrup A, Moesgaard F, Kjaergård J. Fibrin adhesive in the treatment of perineal fistulas. Dis Colon Rectum. 1991. 34:752–754.14. Garcia-Aguilar J, Belmonte C, Wong WD, Goldberg SM, Madoff RD. Anal fistula surgery. Factors associated with recurrence and incontinence. Dis Colon Rectum. 1996. 39:723–729.15. Sentovich SM. Fibrin glue for anal fistulas: long-term results. Dis Colon Rectum. 2003. 46:498–502.16. Park JJ, Cintron JR, Orsay CP, Pearl RK, Nelson RL, Sone J, et al. Repair of chronic anorectal fistulae using commercial fibrin sealant. Arch Surg. 2000. 135:166–169.17. Lindsey I, Smilgin-Humphreys MM, Cunningham C, Mortensen NJ, George BD. A randomized, controlled trial of fibrin glue vs. conventional treatment for anal fistula. Dis Colon Rectum. 2002. 45:1608–1615.18. Chan KM, Lau CW, Lai KK, Auyeung MC, Ho LS, Luk HT, et al. Preliminary results of using a commercial fibrin sealant in the treatment of fistula-in-ano. J R Coll Surg Edinb. 2002. 47:407–410.19. Cintron JR, Park JJ, Orsay CP, Pearl RK, Nelson RL, Sone JH, et al. Repair of fistulas-in-ano using fibrin adhesive: long-term follow-up. Dis Colon Rectum. 2000. 43:944–949.20. Loungnarath R, Dietz DW, Mutch MG, Birnbaum EH, Kodner IJ, Fleshman JW. Fibrin glue treatment of complex anal fistulas has low success rate. Dis Colon Rectum. 2004. 47:432–436.21. Singer M, Cintron J, Nelson R, Orsay C, Bastawrous A, Pearl R, et al. Treatment of fistulas-in-ano with fibrin sealant in combination with intra-adhesive antibiotics and/or surgical closure of the internal fistula opening. Dis Colon Rectum. 2005. 48:799–808.22. Chung CS, Lee DK, George BD, Mortensen NJ. Clinical outcome of a rectovaginal fistula in crohn's disease. J Korean Soc Coloproctol. 2007. 23:10–15.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bronchoscopic Treatment of a Bronchopleural Fistula with using Coils and Fibrin Glue: A case report
- A Case of Bronchoscopic Treatment of a Bronchopleural Fistula Accompanied by Pneumonia
- The Effect of Additional Factor XIII on Cross-linking in Fibrin Glue
- Treatment of a Recurrent Rectourethral Fistula by Using Transanal Rectal Flap Advancement and Fibrin Glue: A Case Report
- Intractable Cerebrospinal Fluid Fistula Following Anterior Decompression in a Patient with Ossifiation of the Posterior Longitudinal Ligament of the Cervical Spine
