Mechanized Posterior Capsulectomy During Combined Vitrectomy and Cataract Surgery
- Affiliations
-
- 1Department of Ophthalmology, College of Medicine Soonchunhyang University, Seoul, Korea. wismile@unitel.co.kr
- KMID: 2210986
- DOI: http://doi.org/10.3341/jkos.2007.48.10.1335
Abstract
-
PURPOSE: To analyze the effects and the stability of a posterior capsulectomy during combined vitrectomy and cataract surgeries in patients with retinal disease.
METHODS
Between 2003 and 2005, the records of patients who underwent posterior capsulectomy during a combined vitrectomy and cataract surgery were followed for 12 months. Among 26 total eyes (17 were from males and nine from females), the average age was 63. An epiretinal membrane was found in 18 eyes, branch retinal vein occlusion in three eyes, diabetic macular edema and vitreous opacity in two eyes, and a macular hole in one eye. The posterior capsulotomy was made smaller than the optic using a vitrectomy cutter after insertion of a posterior chamber intraocular lens (IOL). We investigated postoperative visual acuity, inflammation, and complications.
RESULTS
There were no intraoperative complications. One month postoperatively, one eye (3.8%) showed an increase in intraocular pressure of more than 30 mmHg, one eye (3.8%) showed 2+ inflammatory cells in the anterior chamber. Visual acuity increased by 2 lines postoperatively in 13 eyes (50.0%), whereas visual acuity decreased by more than 1 line in one eye (3.8%). There was a slight decenteration of IOL within 1 mm in two eyes (7.7%) and there was no reclosure of the posterior capsulectomy one year postoperatively.
CONCLUSIONS
Posterior capsulectomy during combined vitrectomy and cataract surgery in patients with retinal disease was simple, safe, and effective in preventing after cataract.
MeSH Terms
Figure
-
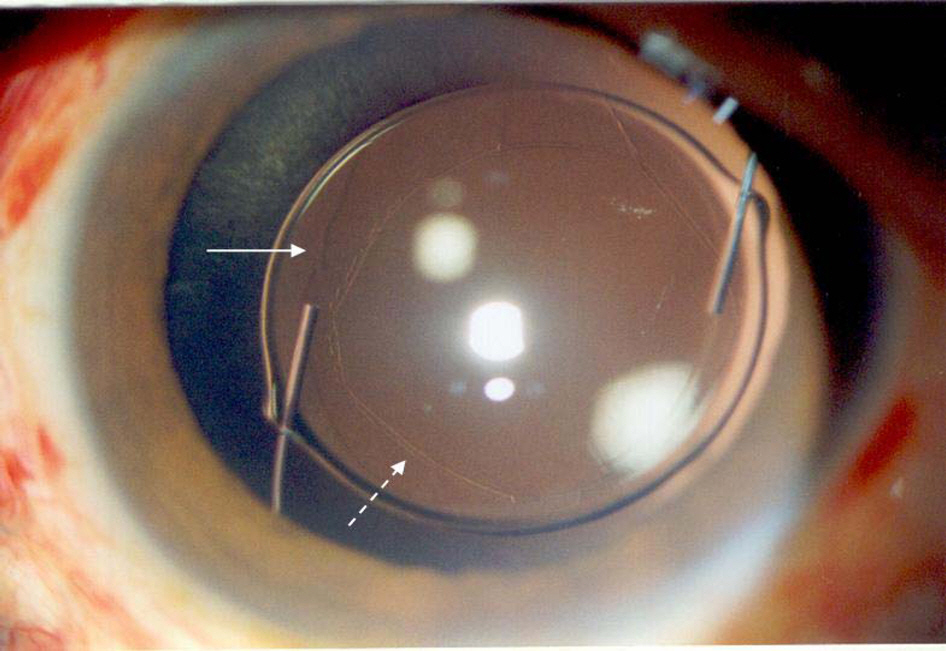
Figure 1. Anterior segment photograph shows anterior (linear arrow) and posterior capsulotomy lines (dotted arrow) at 1 day postoperatively. The posterior capsulotomy was done during combined vitrectomy and cataract operation.
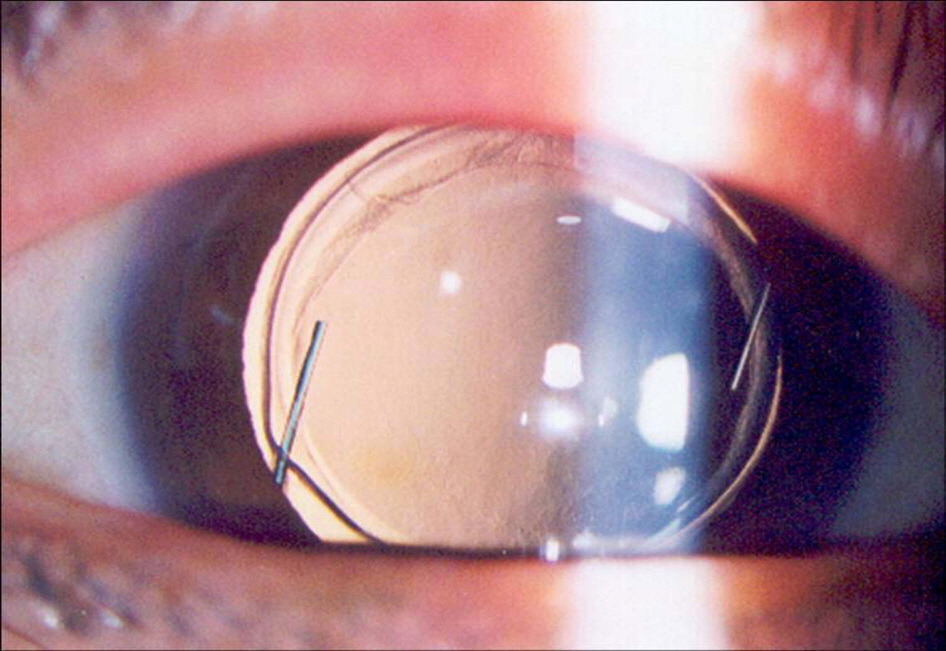
Figure 2. Anterior segment photograph shows mild marginal opacity of the anterior and posterior capsules but clear central view 1 year after posterior capsulotomy during combined vitrectomy and cataract operation.
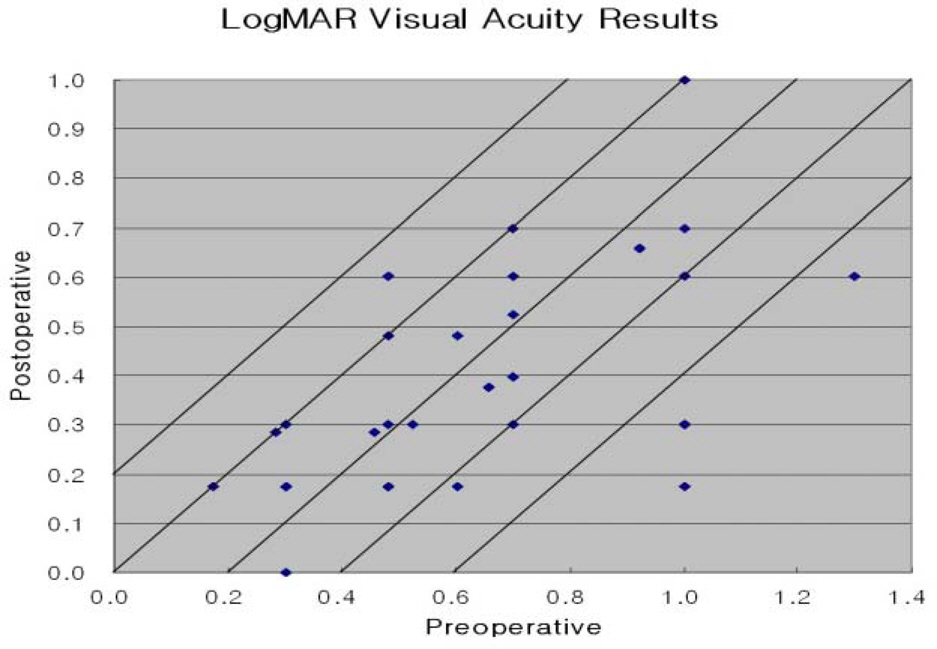
Figure 3. LogMAR visual acuity results (n=26).
Cited by 2 articles
-
Pars Plana Vitrectomy Combined With Surgical Removal of Anterior and Posterior Capsular Opacity
Hae Jung Sun, Kyung Seek Choi, Sung Jin Lee
J Korean Ophthalmol Soc. 2009;50(9):1341-1347. doi: 10.3341/jkos.2009.50.9.1341.Postoperative Refractive Errors after Posterior Capsulectomy during Combined Vitrectomy and Cataract Surgery
Jung Hoon Kim, Sang Beom Han, Seung Jun Lee, Moo Sang Kim
J Korean Ophthalmol Soc. 2015;56(5):709-714. doi: 10.3341/jkos.2015.56.5.709.
Reference
-
References
1. Kappelhof JP, Vrensen GFJM. The Pathology of after cataract; a minireview. Acta Ophthalmol. 1992; 205:S13–24.2. McDonnell PJ, Zarbin MA, Green WR. Posterior capsule opacification in pseudophakic eyes. Ophthalmology. 1983; 90:1548–53.
Article3. Davison JA. Neodymium:YAG laser posterior capsulotomy after implantation of AcrySof intraocular lenses. J Cataract Refract Surg. 2004; 30:1492–500.
Article4. Steinert RF, Puliafito CA, Kumar SR, et al. Cystoid macular edema, retinal detachment, and glaucoma after ND:YAG laser posterior capsulotomy. Am J Ophthalmol. 1991; 112:373–80.
Article5. Stark WJ, Worthen D, Holladay JT, Murray G. Neodymium: YAG lasers; an FDA report. Ophthalmology. 1985; 92:209–12.6. Bath PE, Fankhauser F. Long-term results of ND:YAG laser posterior capsulotomy with the Swiss laser. J Cataract Refract Surg. 1986; 12:150–3.
Article7. Kumagai K, Ogino N, Shinjo U, et al. Vitreous opacification after neodymium :YAG posterior capsulotomy. J Cataract Refract Surg. 1999; 7:981–4.8. Lewis H, Singer TR, Hanscom TA, Straatsma BR. A prospective study of cystoid macular edema after Neodymium:YAG laser posterior capsulotomy. Ophthalmology. 1987; 94:478–82.
Article9. Leff SR, Welch JC, Tasman W. Rhegmatogenous retinal detachment after YAG laser posterior capsulotomy. Ophthalmology. 1987; 94:1222–5.
Article10. Piest KL, Kincaid MC, Tetz MR, et al. Localized endophthalmitis: a newly described cause of the so-called toxic lens syndrome. J Cataract Refract Surg. 1987; 13:498–510.
Article11. Meisler DM, Palestine AG, Vastine DW, et al. Chronic Propionibacterium endophthalmitis after extracapsular cataract extraction and intraocular lens implantation. Am J Ophthalmol. 1986; 102:733–9.
Article12. Gimbel HV, Neuhann T. Development, advantages and methods of continuous circular capsulorhexis technique. J Cataract Refract Surg. 1990; 16:31–7.13. Gimble HV. Posterior continuous curvilinear capsulorhexis and optic capture of the intraocular lens to prevent secondary opacification in pediatric cataract surgery. J Cataract Refract Surg. 1997; 23:652–6.14. Galand A, van Cauwenberge F, Moosavi J. Posterior capsulorhexis in adult eyes with intact and clear capsules. J Cataract Refract Surg. 1996; 22:458–61.
Article15. Ryu CH, Kim HB, Lim SJ. Clinical result of planned posterior continuous curvilinear capsulorrhexis in adult cataract patients: 1 year follow-up. J Korean Ophthalmol Soc. 2000; 41:2547–54.16. Menapace R. Routine posterior optic buttonholing for eradication of posterior capsule opacification in adults: Report of 500 consecutive cases. J Cataract Refract Surg. 2006; 32:929–43.17. Kim SH, Chung JW, Chung H, Yu HG. Phacoemulsification and foldable intraocular lens implantation combined with vitrectomy and silicone oil tamponade for severe proliferative diabetic retinopathy. J Cataract Refract Surg. 2004; 30:1721–6.
Article18. Weinreb RN, Wasserstrom JP, Parker W. Neovascular glaucoma following Neodyamium-YAG laser posterior capsulotomy. Arch Ophthalmol. 1986; 104:730–1.19. Poliner LS, Christionason DJ, Escoffery RF, et al. Neovascular glaucoma after intracapsular and extracapsular cataract extraction in diabetic patients. Am J Ophthalmol. 1985; 100:637–43.
Article20. Suthakar J, Ravindron RD, Natchiar G. Analysis of complication in 100 cases of posterior chamber intraocular lens implantation. Indian J Ophthalmol. 1989; 37:78–9.21. Pollack A, Leiba H, Bukelman A, Olivvier M. Cystoid macular oedema following cataract extraction in patients with diabetes. Br J Ophthalmol. 1992; 76:221–4.
Article22. Hooper PL, Rao HA, Smith RE. Cataract extraction in uveitis patients. Surv Ophthalmol. 1990; 35:120–44.
Article23. Ionides A, Dowler JG, Hykin PG, et al. Posterior capsule opacification following diabetic extracapsular cataract extraction. Eye. 1994; 8:120–144.
Article24. Toda J, Kato S, Oshika T, Sugita G. Posterior capsule opacification after combined cataract surgery and vitrectomy. J Catarct Refract Surg. 2007; 33:104–7.
Article25. Yang X, Zou L, Binrong M, et al. Tensile strength of lens capsules in eye-bank eyes. J Cataract Refract Surg. 1998; 24:543–6.
Article26. Krag S, Thim K, Corydon L. Strength of the lens capsule during hydroexpression of the nucleus. J Cataract Refract Surg. 1993; 19:666–7.
Article27. Krag S, Andereassen TT. Mechanical properties of the human posterior lens capsule. Invest Ophthalmol Vis Sci. 2003; 44:691–6.
Article28. Wilson ME, Saunders RA, Roberts EL, Apple DJ. Mechanized anterior capsulectomy as an alternative to manual capsulorhexis in children undergoing intraocular lens implantation. J Pediatr Ophthalmol Strabismus. 1996; 33:237–40.
Article29. Tassignon MJ, De Groot V, Smets RM. Secondary closure of posterior continuous curvilinear capsulorhexis. J Cataract Refract Surg. 1996; 22:1200–5.
Article30. Tassignon MJ, De Groot V, Vervecken F, Tenten YV. Secondary closure of posterior continuous curvilinear capsulorhexis in normal eyes and eyes at risk for postoperative inflammation. J Cataract Refract Surg. 1998; 24:1333–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postoperative Refractive Errors after Air Tamponade with Posterior Capsulectomy during Combined Vitrectomy and Cataract Surgery
- Postoperative Refractive Errors after Posterior Capsulectomy during Combined Vitrectomy and Cataract Surgery
- Effect of Posterior Chamber Intraocular Lens Implantation on Unilateral Pediatric Cataract
- The effect of posterior continuous circular capsulectomy with anterior vitrectomy in pediatric cataract on development of posterior capsular opacification
- Treatment and Prognosis of Cataract in Children
