Case Report of Arm Kimura Disease with Atypical MR Finding
- Affiliations
-
- 1Department of Radiology, Korea University Ansan Hospital, Korea University College of Medicine, Korea. kimbaekh@hanmail.net
- 2Department of Radiology, Korea University Guro Hospital, Korea University College of Medicine, Korea.
- 3Department of Radiology, Korea University Anam Hospital, Korea University College of Medicine, Korea.
- 4Department of Pathology, Korea University Ansan Hospital, Korea University College of Medicine, Korea.
- KMID: 2208924
- DOI: http://doi.org/10.3348/jksr.2010.62.3.277
Abstract
- Kimura disease is a rare chronic inflammatory condition of unknown origin that occurs mainly in young Asian male patients. Kimura disease is characterized by painless subcutaneous swelling and lymphadenopathy of the head and neck, associated with peripheral blood eosinophilia and increased serum IgE. According to some previous reports about a rare form of Kimura disease of the upper arm, soft tissue masses of the subcutaneous fat layer were demonstrated in the medial trochlear area, which showed strong and homogenous enhancement with marked perilesional edema and fat infiltrations on enhanced magnetic resonance imaging (MRI). In this case report, we introduce a case of Kimura disease of the upper arm in a 13-year male patient, which was seen as a well-marginated soft tissue mass without perilesional edema or fatty infiltrations on MRI. In this case study, we discuss the characteristics of the clinical and pathologic findings associated with unusual MRI findings, and report the Kimura disease with a different pathophysiology by anti-inflammatory drugs.
MeSH Terms
Figure
-

Fig. 1 A. A well-marginated, elliptical soft tissue mass was identified in medial epitrochlear area of left upper arm, which showed low echogenicity with an echogenic hilum on US. It measured about 5.5×1.5×1.3 cm in size. B. On color Doppler US, increased vascularity was seen along hilum of lymph node.
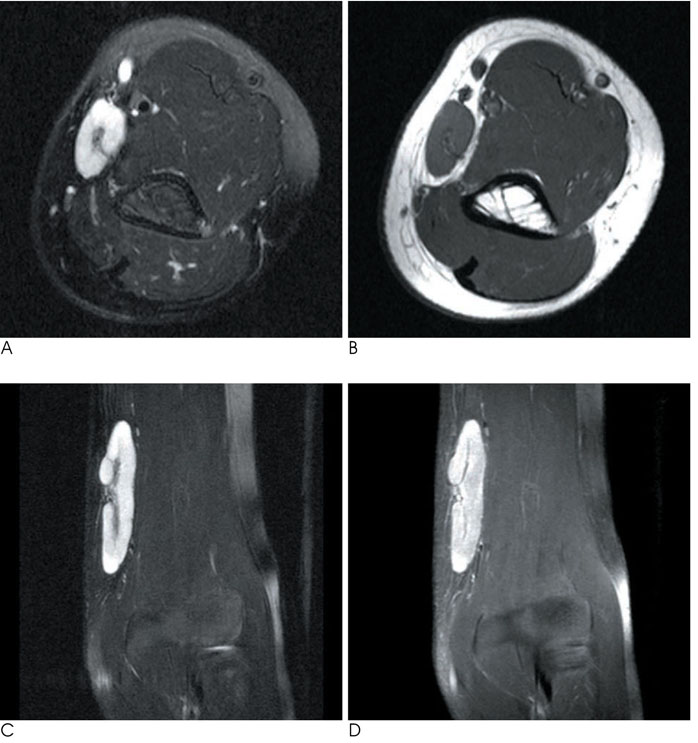
Fig. 2 A. Axial fat supressed T2-weighted (TR/TE, 3389/96) spin-echo MR image showed well-defined homogeneous high signal intensity mass located in medial epitrochlear area of left upper arm. B. Axial T1-weighted image (TR/TE, 459/12) showed good demarcation around the mass. C. A well-defined enlongated mass, located in medial epitrochlear area of left upper arm, showed homogeneous high signal intensity on coronal fat-supressed T2-weighted image (TR/TE, 3389/96) with branching low signal intensity along hilum. There was neither perilesional edema nor fat infiltration. D. After intravenous gadolinium enhancement, the mass was enhanced strongly and homogeneously. There was no evidence of perilesional edema or fat infiltration.
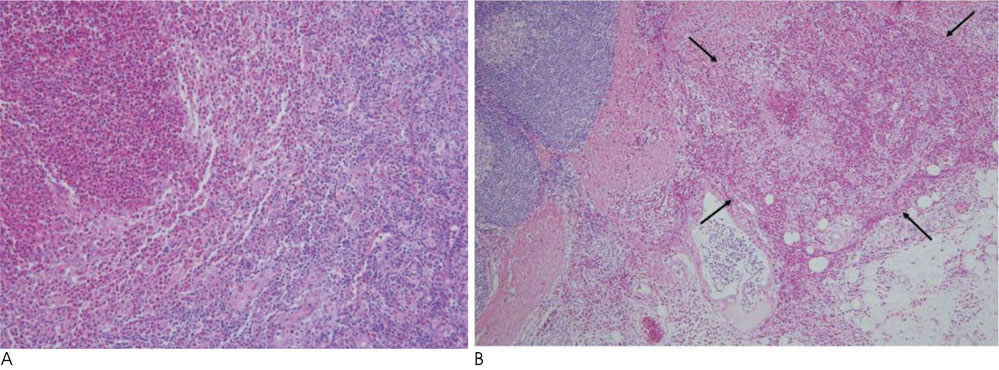
Fig. 3 A. On microscopic evaluation, there were lymphoid follicular hyperplasia and vascular proliferations with extensive infiltration of mature eosinophils in the mass, which was compatible with microscopic findings of Kimura disease (H & E, ×200). B. There was a focal, localized eosinophilic infiltration around the outer margin of the mass measured about 1×1 mm (arrows, H & E, ×100).
Reference
-
1. Ginsberg LE, McBride JA. Kimura's disease. AJR Am J Roentgenol. 1998; 171:1508.2. Choi JA, Lee GK, Kong KY, Hong SH, Suh JS, Ahn JM, et al. Imaging findings of kimura's disease in the soft tissue of the upper extremity. AJR Am J Roentgenol. 2005; 184:193–199.3. Kim H, Szeto C. Eosinophilic hyperplastic lymphogranuloma, comparison with mikulicz's disease. Chin Med J. 1937; 23:699–700.4. Kimura T, Yoshimura S, Ishikawa E. Unusual granulation combined with hyperplastic changes in lymphatic tissue. Trans Soc Pathol Jpn. 1948; 37:179–180.5. Takahashi S, Ueda J, Furukawa T, Tsuda M, Nishimura M, Orita H, et al. Kimura disease: CT and MR findings. AJNR Am J Neuroradiol. 1996; 17:382–385.6. Smith JR, Hadgis C, Van Hasselt A, Metreweli C. CT of kimura disease. AJNR Am J Neuroradiol. 1989; 10:S34–S36.7. Som PM, Biller HF. Kimura disease involving parotid gland and cervical nodes: CT and MR findings. J Comput Assist Tomogr. 1992; 16:320–322.8. Lim WE, Tan NG, Tan KP. Radiological features in a patient with kimura's disease. Singapore Med J. 1997; 38:125–128.9. Park JS, Jin W, Ryu KN, Won KY. Bilateral asymmetric superficial soft tissue masses with extensive involvement of both upper extremities: demonstration of kimura's disease by US and MRI (2008: 12b). Eur Radiol. 2009; 19:781–786.10. Dong PR, Seeger LL, Yao L, Panosian CB, Johnson BL Jr, Eckardt JJ. Uncomplicated cat-scratch disease: findings at CT, MR imaging, and radiography. Radiology. 1995; 195:837–839.
