Correlation between Computed Tomography and Pathological Findings of Gastrointestinal Stromal Tumors Treated with Imatinib Mesylate
- Affiliations
-
- 1Department of Radiology, Anam Hospital, College of Medicine, Korea University, Seoul, Korea. radiolbj226@gmail.com
- 2Department of Radiology, Asan Medical Center, College of Medicine, University of Ulsan, Seoul, Korea.
- 3Department of Imaging Medicine, College of Medicine, Kangwon National University, Chuncheon, Korea.
- KMID: 2208793
- DOI: http://doi.org/10.3348/jksr.2014.71.5.239
Abstract
- PURPOSE
To evaluate the correlation between pathological and computed tomography (CT) findings of gastrointestinal stromal tumors (GISTs) after imatinib mesylate (imatinib) treatment.
MATERIALS AND METHODS
Twenty-six patients with GIST (17 men, 9 women; mean age, 56 years) who underwent treatment with imatinib and who were registered at our institution were included. Eight patients had primary and 18 had metastatic tumors. The correlation between CT and pathological findings was evaluated for all 26 tumors, which were resected after imatinib treatment.
RESULTS
The mean size change in the tumors after imatinib treatment was -1.4 cm (range, -7.8-2.5 cm). A reduction in tumor CT attenuation value was observed after imatinib treatment (mean, 29.1 Hounsfield units) in 20 of 26 tumors. Reduced attenuation was associated with non-tumorous pathological findings, including cystic degeneration (6/20), hemorrhagic necrosis (6/20), hyaline degeneration (6/20), and combined pathology without a viable portion (2/20). Of six tumors showing increased attenuation values after treatment, four (66.7%) showed an abundant viable portion. The increase in tumor size was not associated with the presence of a viable portion in any tumor.
CONCLUSION
CT attenuation changes in GISTs may adequately reflect the pathological findings in GISTs after imatinib treatment.
MeSH Terms
Figure
-

Fig. 1 Transverse CT scans of a gastrointestinal stromal tumor before and after imatinib treatment in a 36-year-old man. CT attenuation was measured by adjusting the rectangular region of interest to encompass as much as possible of the portion showing a significant change in CT findings before and after imatinib treatment. A. Solid mass with lobulated contour abutting the small bowel before imatinib treatment. B. Six months after imatinib treatment, the attenuation of the solid tumor had decreased, and a peripheral wall and internal septation were apparent. C. Gross specimen showing the resected small bowel and large bowel loops with the chamber of cystic degeneration (solid arrow). D. Microscopic examination revealed extensive multiloculated cystic degeneration (Cy) with an internal septum containing viable tumor cells (Vi) (H&E stain, × 20).

Fig. 2 Transverse CT scans of a primary gastrointestinal stromal tumor (GIST) of the small bowel in a 53-year-old man. A. A CT scan before imatinib treatment shows a heterogeneous low attenuated mass abutting pelvic ileal loops. B. CT scans obtained 18 months after imatinib treatment showed a lesion with reduced attenuation, suggestive of a cyst-like component with an intramural nodule (solid arrow). C. Photograph of a resected and opened GIST from the ileum showing a central cavity in the gross specimen. D. Microscopic examination revealed extensive hemorrhagic necrosis (HN) (H&E stain, × 40).

Fig. 3 Transverse CT scans of a splenic metastasis from a gastrointestinal stromal tumor of the stomach in a 62-year-old woman. A. A CT scan before imatinib treatment reveals a heterogeneous, hypo-attenuated metastatic lesion in the spleen. B. A CT scan obtained 28 months after imatinib treatment. The metastatic spleen lesion is nearly resolved, and the cystic lesion including ascites and fluid collection has developed next to the spleen (open arrow). C. Photomicrograph of the resected spleen. Hyaline changes owing to ascites or fluid collection outside the splenic capsule (solid arrows) and splenic parenchyma (*) are not a true cystic degeneration but extensive hyalinization (Hy) (H&E stain, × 20).

Fig. 4 Transverse CT scans of a primary gastrointestinal stromal tumor (GIST) of the stomach in a 68-year-old man. A. A CT scan before imatinib treatment showed a heterogeneously attenuated GIST arising in the stomach. B. A CT scan obtained 27 months after imatinib treatment reveals a homogenous lesion with reduced attenuation and extensive internal calcification (solid arrow). The dominant gross and microscopic pathological finding was of hyalinization with abundant calcification.
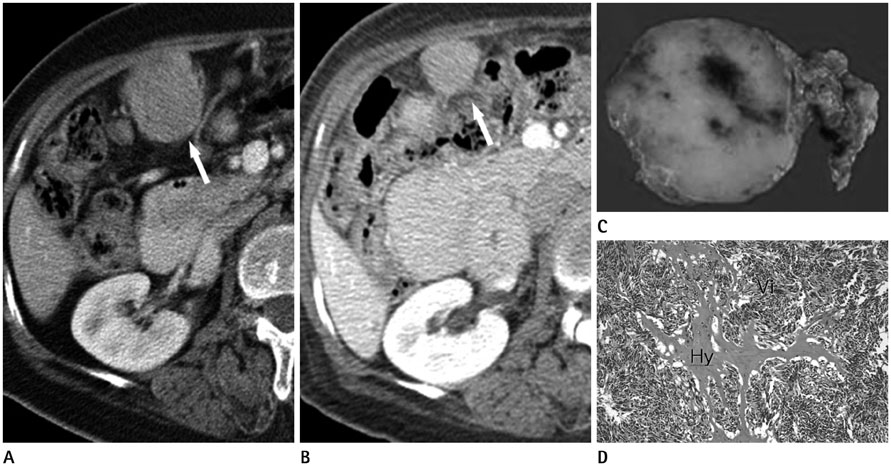
Fig. 5 Transverse CT scans of omental metastasis from gastrointestinal stromal tumor of small bowel in 64-year-old woman. A. A CT scan before imatinib treatment showing highly attenuated heterogeneous round mass beside hepatic flexure of the colon (solid arrow). B. A CT scan 14 months after imatinib treatment reveals a metastatic lesion (solid arrow). The size has decreased with an increase of homogeneity in internal attenuation. C. Gross specimen of resected omental mass showing solid mass with minimal internal hemorrhage in the cut surface. D. Photomicrograph of resected omental mass showing spindle-shaped hypercellular viable tumor (Vi) in most part of tumor with interspersed hyalinization (Hy). The viable tumor portion and the interspersed hyalinization with scanty hemorrhage occupied in about 75% and 25% of the tumor, respectively (H&E stain, × 100).
Reference
-
1. George S, Desai J. Management of gastrointestinal stromal tumors in the era of tyrosine kinase inhibitors. Curr Treat Options Oncol. 2002; 3:489–496.2. DeMatteo RP, Lewis JJ, Leung D, Mudan SS, Woodruff JM, Brennan MF. Two hundred gastrointestinal stromal tumors: recurrence patterns and prognostic factors for survival. Ann Surg. 2000; 231:51–58.3. Roberts PJ, Eisenberg B. Clinical presentation of gastrointestinal stromal tumors and treatment of operable disease. Eur J Cancer. 2002; 38:Suppl 5. S37–S38.4. Lehnert T. Gastrointestinal sarcoma (GIST)--a review of surgical management. Ann Chir Gynaecol. 1998; 87:297–305.5. Judson I. Gastrointestinal stromal tumours (GIST): biology and treatment. Ann Oncol. 2002; 13:Suppl 4. 287–289.6. Pidhorecky I, Cheney RT, Kraybill WG, Gibbs JF. Gastrointestinal stromal tumors: current diagnosis, biologic behavior, and management. Ann Surg Oncol. 2000; 7:705–712.7. Dennis KL, Damjanov I. Evaluating and reporting gastrointestinal stromal tumors after imatinib mesylate treatment. Open Pathol J. 2009; 3:53–57.8. Sarlomo-Rikala M, Kovatich AJ, Barusevicius A, Miettinen M. CD117: a sensitive marker for gastrointestinal stromal tumors that is more specific than CD34. Mod Pathol. 1998; 11:728–734.9. Eisenberg BL, Judson I. Surgery and imatinib in the management of GIST: emerging approaches to adjuvant and neoadjuvant therapy. Ann Surg Oncol. 2004; 11:465–475.10. Dematteo RP, Ballman KV, Antonescu CR, Maki RG, Pisters PW, Demetri GD, et al. Adjuvant imatinib mesylate after resection of localised, primary gastrointestinal stromal tumour: a randomised, double-blind, placebo-controlled trial. Lancet. 2009; 373:1097–1104.11. Choi H. Critical issues in response evaluation on computed tomography: lessons from the gastrointestinal stromal tumor model. Curr Oncol Rep. 2005; 7:307–311.12. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan RS, Rubinstein L, et al. European Organization for Research and Treatment of Cancer. National Cancer Institute of the United States. National Cancer Institute of Canada. New guidelines to evaluate the response to treatment in solid tumors. J Natl Cancer Inst. 2000; 92:205–221.13. Benjamin RS, Choi H, Macapinlac HA, Burgess MA, Patel SR, Chen LL, et al. We should desist using RECIST, at least in GIST. J Clin Oncol. 2007; 25:1760–1764.14. Choi H, Charnsangavej C, de Castro Faria S, Tamm EP, Benjamin RS, Johnson MM, et al. CT evaluation of the response of gastrointestinal stromal tumors after imatinib mesylate treatment: a quantitative analysis correlated with FDG PET findings. AJR Am J Roentgenol. 2004; 183:1619–1628.15. Schiavon G, Ruggiero A, Schoffski P, van der Holt B, Bekers DJ, Eechoute K, et al. Tumor volume as an alternative response measurement for imatinib treated GIST patients. PLoS One. 2012; 7:e48372.16. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010; 30:52–60.17. Choi H, Faria S, Benjamin R, Podoloff D, Macapinlac H, Charnsangavej C. Monitoring treatment effects of STI-571 on gastrointestinal stromal tumors (GIST) with CT and PET: a quantitative analysis. Chicago, IL: Presented at Radiological Society of North America Scientific Program;2002.18. Prasad SR, Jhaveri KS, Saini S, Hahn PF, Halpern EF, Sumner JE. CT tumor measurement for therapeutic response assessment: comparison of unidimensional, bidimensional, and volumetric techniques initial observations. Radiology. 2002; 225:416–419.19. Hong X, Choi H, Loyer EM, Benjamin RS, Trent JC, Charnsangavej C. Gastrointestinal stromal tumor: role of CT in diagnosis and in response evaluation and surveillance after treatment with imatinib. Radiographics. 2006; 26:481–495.20. Kim HC, Lee JM, Choi SH, Han H, Kim SS, Lee SH, et al. Cystic changes in intraabdominal extrahepatic metastases from gastrointestinal stromal tumors treated with imatinib. Korean J Radiol. 2004; 5:157–163.21. Chen MY, Bechtold RE, Savage PD. Cystic changes in hepatic metastases from gastrointestinal stromal tumors (GISTs) treated with Gleevec (imatinib mesylate). AJR Am J Roentgenol. 2002; 179:1059–1062.22. Oh JS, Lee JL, Kim MJ, Ryu MH, Chang HM, Kim TW, et al. Neoadjuvant imatinib in locally advanced gastrointestinal stromal tumors of the stomach: report of three cases. Cancer Res Treat. 2006; 38:178–183.23. Bechtold RE, Chen MY, Stanton CA, Savage PD, Levine EA. Cystic changes in hepatic and peritoneal metastases from gastrointestinal stromal tumors treated with Gleevec. Abdom Imaging. 2003; 28:808–814.24. Reynoso D. Bim mediates imatinib-induced apoptosis of gastrointestinal stromal tumors: Translational implications. UT GSBS Dissertations and Theses (Open Access). 2012. p. 11–12.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imatinib-induced hepatitis treated by corticosteroids in a patient with metastatic gastrointestinal stromal tumor
- Two different KIT mutations may lead to different responses to imatinib in metastatic gastrointestinal stromal tumor
- A Case of Generalized Keratosis Pilaris Induced by Imatinib Mesylate
- Postoperative Cure for Metastatic Gastrointestinal Stromal Tumor
- Imatinib-induced DRESS Syndrome in Gastrointestinal Stromal Tumor
