J Korean Soc Transplant.
2015 Sep;29(3):170-174. 10.4285/jkstn.2015.29.3.170.
Adult Kidney Transplantation of Pediatric En bloc Kidneys Using a Partial Bladder Wall
- Affiliations
-
- 1Department of Transplantation Surgery, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. KHHUH@yuhs.ac
- 2Department of Urology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2202590
- DOI: http://doi.org/10.4285/jkstn.2015.29.3.170
Abstract
- Kidney transplantation is a treatment of choice which improves survival and quality of life for patients with end-stage renal disease. Due to the growing waiting list for kidney transplantation, expansion of the donor pool to use of deceased pediatric kidneys is of critical importance. However, the use of pediatric kidneys has been limited due to concerns about early graft failure, hyperfiltration injury, and technical difficulties. Performing ureteroneocystostomy using small pediatric en bloc kidneys is sometimes difficult due to the small diameter and short length of the ureter in the adult kidney recipient. We hereby report on a partial bladder wall transplantation using pediatric en bloc kidneys. Pediatric en bloc kidneys and partial bladder wall from a 12-month-old female donor who weighed 9.13 kg was transplanted into a 49-year-old male recipient. The urinary tract was reconstructed with a partial bladder wall of the donor. At 12 months post-transplantation, Doppler ultrasonograpy and renogram showed stable graft renal function without urological complications. Pediatric en bloc kidney transplantation with a partial bladder wall can be a safe and feasible surgical technique to reduce urological complications.
MeSH Terms
Figure
-

Fig. 1. (A) Pediatric en bloc kidneys with ureters and partial bladder segment. (B) Reconstruction of urinary tract with a partial bladder wall of the donor.

Fig. 2. (A, B) Implantation of en bloc kidneys with partial bladder segment.
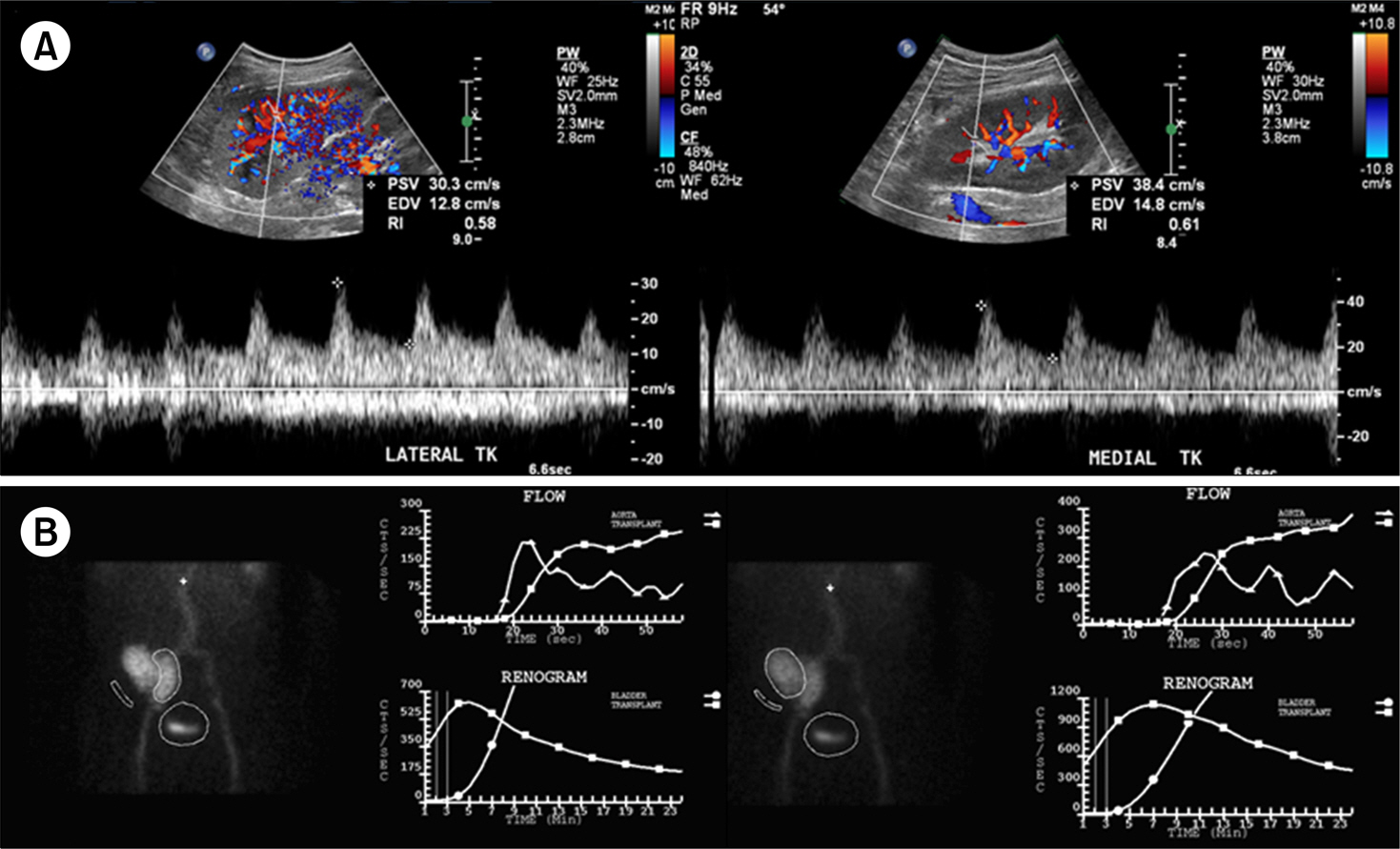
Fig. 3. (A) Doppler ultrasonogram (U/S) image. Doppler U/S shows normal resistant index and vascularity. (B) Renogram image, renogram scan shows normal limits of blood flow and function.
Reference
-
References
1). Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999; 341:1725–30.
Article2). Korean Network for Organ Sharing (KONOS). 2013 KONOS Annual Report [Internet]. Seoul: KONOS;2014. [cited 2015 Apr 5]. Available from:. http://www.konos.go.kr.3). Korean Network for Organ Sharing (KONOS). KONOS Data [Internet]. Seoul: KONOS;2014. [cited 2015 Apr 5]. Available from:. http://www.konos.go.kr.4). Sureshkumar KK, Reddy CS, Nghiem DD, Sandroni SE, Carpenter BJ. Superiority of pediatric en bloc renal allografts over living donor kidneys: a longterm functional study. Transplantation. 2006; 82:348–53.5). Terasaki PI, Koyama H, Cecka JM, Gjertson DW. The hyper-filtration hypothesis in human renal transplantation. Transplantation. 1994; 57:1450–4.
Article6). Kato T, Selvaggi G, Burke G, Ciancio G, Zilleruelo G, Hattori M, et al. Partial bladder transplantation with en bloc kidney transplant: the first case report of a ‘bladder patch technique' in a human. Am J Transplant. 2008; 8:1060–3.7). Snanoudj R, Rabant M, Timsit MO, Karras A, Savoye E, Tricot L, et al. Donor-estimated GFR as an appropriate criterion for allocation of ECD kidneys into single or dual kidney transplantation. Am J Transplant. 2009; 9:2542–51.
Article8). Bresnahan BA, McBride MA, Cherikh WS, Hariharan S. Risk factors for renal allograft survival from pediatric cadaver donors: an analysis of united network for organ sharing data. Transplantation. 2001; 72:256–61.9). Wengerter K, Matas AJ, Tellis VA, Quinn T, Soberman R, Veith FJ. Transplantation of pediatric donor kidneys to adult recipients. Is there a critical donor age? Ann Surg. 1986; 204:172–5.10). Sharma A, Fisher RA, Cotterell AH, King AL, Maluf DG, Posner MP. En bloc kidney transplantation from pediatric donors: comparable outcomes with living donor kidney transplantation. Transplantation. 2011; 92:564–9.
Article11). Maluf DG, Carrico RJ, Rosendale JD, Perez RV, Feng S. Optimizing recovery, utilization and transplantation outcomes for kidneys from small, ≤20 kg, pediatric donors. Am J Transplant. 2013; 13:2703–12.12). Nghiem DD, Hsia S, Schlosser JD. Growth and function of en bloc infant kidney transplants: a preliminary study. J Urol. 1995; 153:326–9.
Article13). Hiramoto JS, Freise CE, Randall HR, Bretan PN, Tomlanovich S, Stock PG, et al. Successful longterm outcomes using pediatric en bloc kidneys for transplantation. Am J Transplant. 2002; 2:337–42.
Article14). Bretan PN Jr, Friese C, Goldstein RB, Osorio RW, Tomlanovich S, Amend W, et al. Immunologic and patient selection strategies for successful utilization of less than 15 kg pediatric donor kidneys: long term experiences with 40 transplants. Transplantation. 1997; 63:233–7.15). Drakopoulos S, Koukoulaki M, Vougas V, Apostolou T, Hadjiyannakis EI, Hadjiconstantinou V. Transplantation of pediatric kidneys to adult recipients: an analysis of 13 cases. Transplant Proc. 2004; 36:3161–3.
Article16). Ahn HJ, Kim JH, Chang HK, Rha KH, Kim YS. Urodynamic evidence of successful rehabilitation of a severely contracted bladder after renal transplantation. Transpl Int. 2007; 20:1074–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transplantation of En Bloc Pediatric Cadaver Kidneys into Adult Recipient
- En bloc transplantation of horseshoe kidney in Korea
- Utility of a Computed Tomography-Based Navigation System (O-Arm) for En Bloc Partial Vertebrectomy for Lung Cancer Adjacent to the Thoracic Spine: Technical Case Report
- Is Pretransplant Bladder Augmentation Using Hydrostatic Pressure of Contracted Bladder in Chronic Renal Failure Really Effective?
- Pediatric Kidney Transplantation
