J Lung Cancer.
2008 Jun;7(1):34-35. 10.6058/jlc.2008.7.1.34.
Esophageal Cancer with Left Main Bronchus Obstruction
- Affiliations
-
- 1Department of Internal Medicine, Chonnam National University Hwasun Hospital, Hwasun, Korea. cyberkks@chonnam.ac.kr
- KMID: 2200071
- DOI: http://doi.org/10.6058/jlc.2008.7.1.34
Abstract
- A 66-year-old man with recurrent esophageal cancer was admitted to our health care facility for evaluation of resting dyspnea. He had undergone an esophagectomy with cervical esophagogastrostomy in May 2007 and had undergone radical radiation treatment from June to August 2007. After 6 months, he complained of cough and dyspnea. A metastatic lymphadenopathy, 4 cm in size, was in the para-aortic space and compressed the left main bronchus, resulting in total atelectasis of the left lung, as demonstrated on follow-up chest simple x-ray and CT (Fig. 1, 2). He initially received one cycle of chemotherapy consisting of docetaxel and cisplatin, but there was no change in the lung atelectasis and the dyspnea had worsened. The decision was therefore made to perform a rigid bronchoscopy. Under general anesthesia, an endobronchial obstructive lesion was removed using a mechanical core-out technique with rigid bronchoscopy (Fig. 3). After the procedure, the atelectasis resolved nearly completely, and neither severe bleeding nor other complications were noted (Fig. 4). The dyspnea was relieved from ATS (American thoracic society) grade 4 to grade 2. Following this treatment, chemotherapy for recurrent esophageal cancer was resumed
Keyword
MeSH Terms
Figure
-
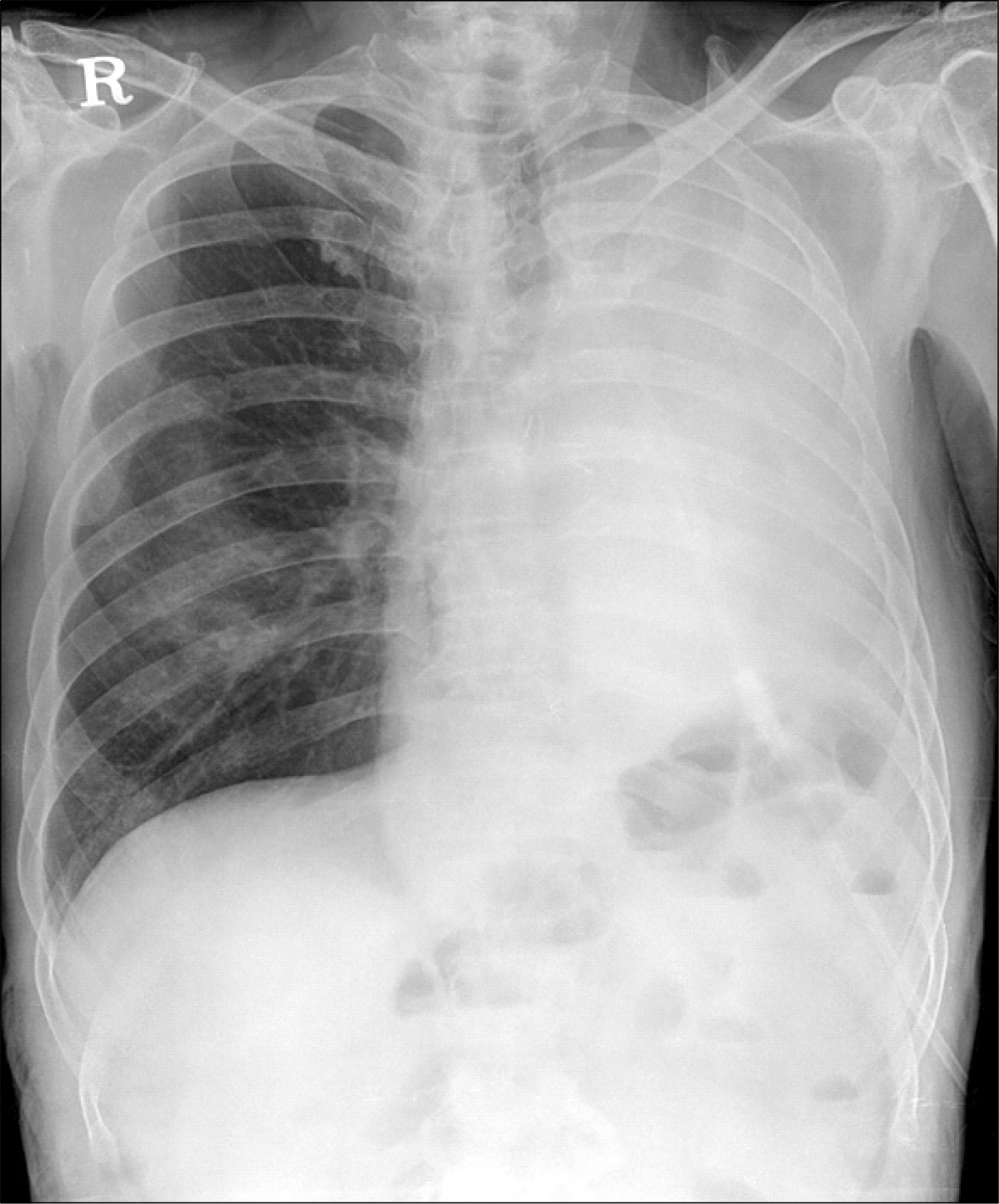
Fig. 1. Plain chest X-ray obtained for evaluation of dyspnea and showed total atelectasis of the left lung.
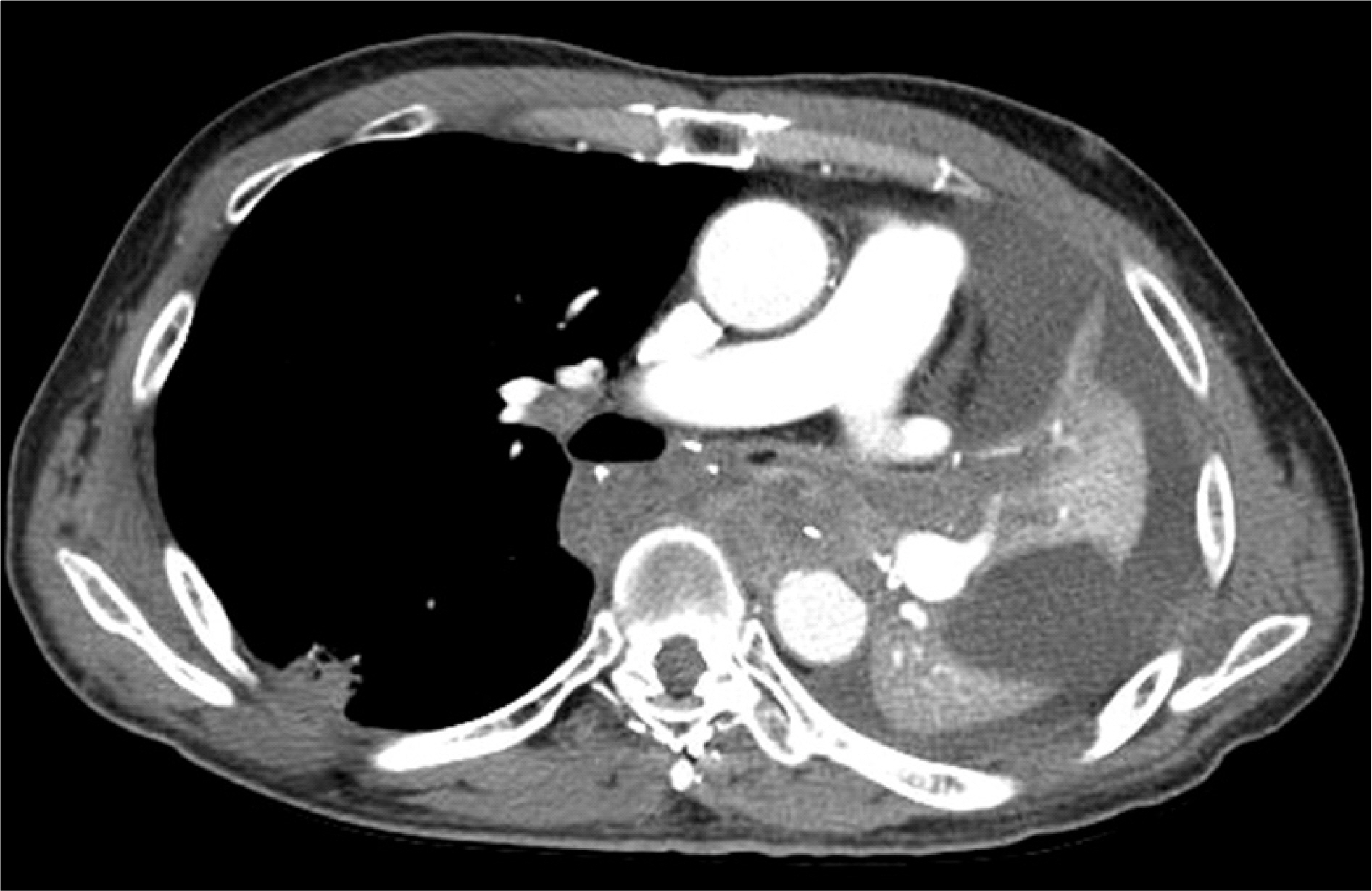
Fig. 2. Chest CT shows a 4 cm necrotizing LAP in the paraaortic space with compression of the left main bronchus, leading to total atelectasis in the left lung.

Fig. 3. Mechanical resection of the endobronchial obstructive lesion using a mechanical core-out technique with rigid bronchoscopy.
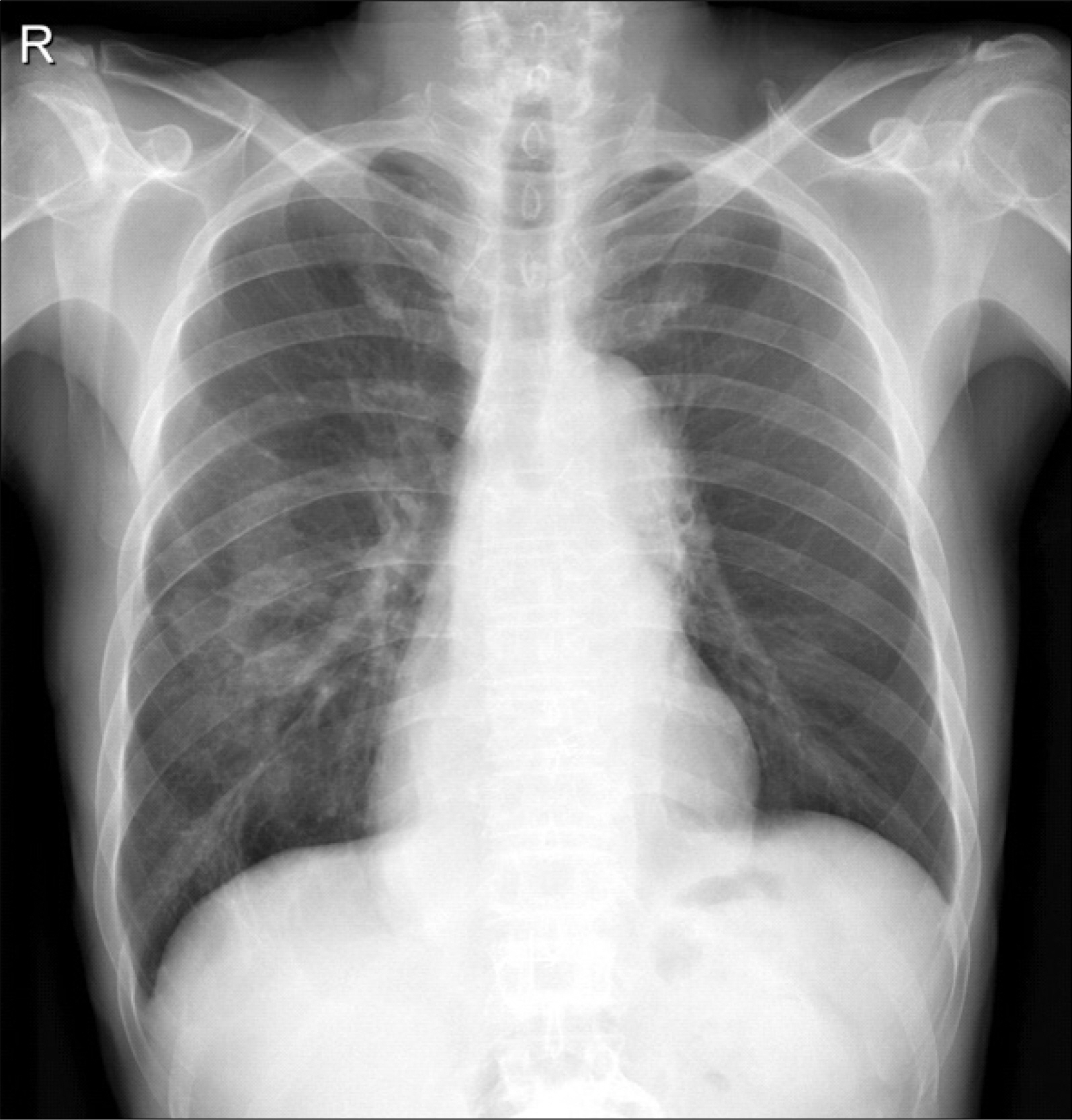
Fig. 4. After the procedure, follow up chest X-ray showed near-complete resolution of the atelectasis and remarkable improvement of aeration in the left lung.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bronchoplastic Procedures after Sleeve Resextion of Left Main Bronchus Including Left Lower Lobe (A Case Report)
- Hemangioendothelioma Leading to Obstruction of the Left Main Bronchus in Infant
- Obstruction of Dependent Bronchus by Necrotic Cancer Materials during Pneumonectomy: A case report
- The Compression of Left Main Bronchus Caused by Dilated Descending Aorta After Ligation of PDA
- Glomus Tumor in Left Main Bronchus: A Case Report
