Conservative management of shoulder pain with common causes
- Affiliations
-
- 1Department of Rehabilitation Medicine, Seoul Metropolitan Government Boramae Medical Center, Seoul National University College of Medicine, Seoul, Korea. shiuk.lee@gmail.com
- KMID: 2194916
- DOI: http://doi.org/10.5124/jkma.2014.57.8.661
Abstract
- Shoulder pain presents with varying etiology and pathophysiology. At the time of initial evaluation, conservative management is applied in most cases. The therapeutic approach should be based on the cause of pain, which should be determined by the appropriate evaluation. Recovery of range of motion, strengthening of rotator cuffs and other shoulder muscles, and scapular stabilization are the main principles and purposes of shoulder rehabilitation. In this article, we introduce diagnosis-specific management approaches for common presentations of shoulder pain such as adhesive capsulitis, impingement syndrome or rotator cuff tendinosis, and calcific tendinitis.
Keyword
MeSH Terms
Figure
-
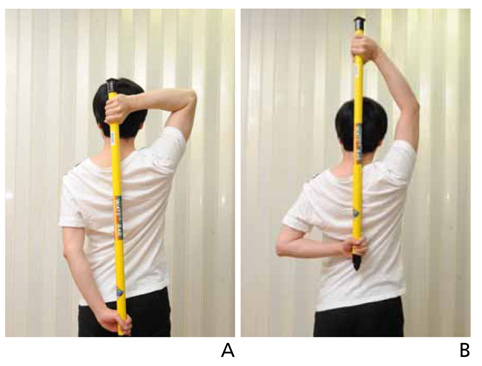
Figure 1 An example of self range-of-motion exercise with a bar. In this photo, passive internal rotation of the left shoulder is performed by gently pulling the bar upwards with the right arm (A,B).
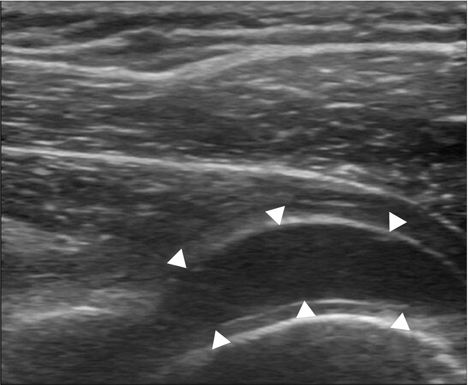
Figure 2 The shoulder capsule is expanded (arrow heads) after intraarticular hydraulic distention.
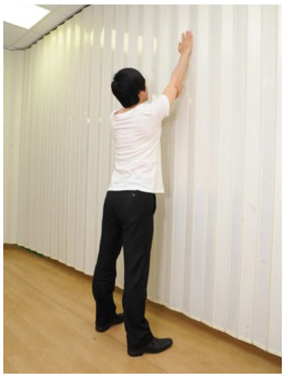
Figure 3 Wall slide exercise is performed by gently pushing the arm upwards against the wall with elbow supported by the other hand. At the end range, the patient is educated to lean towards the wall to further slide the arm upwards.

Figure 4 Rotator cuff strengthening exercise can be done with a theraband, by tying one end at the door knob. The photo shows external rotation exercise (A,B). Informed consent was received from the subject.
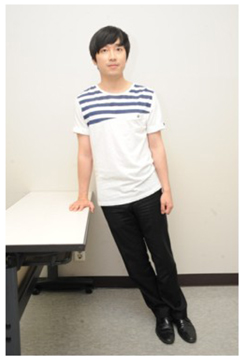
Figure 5 Low row exercise is a basic exercise for scapular stabilization. With the trunk extended and scapula retracted, the patient puts the affected arm extended on a desk and push backwards. Informed consent was received from the subject.
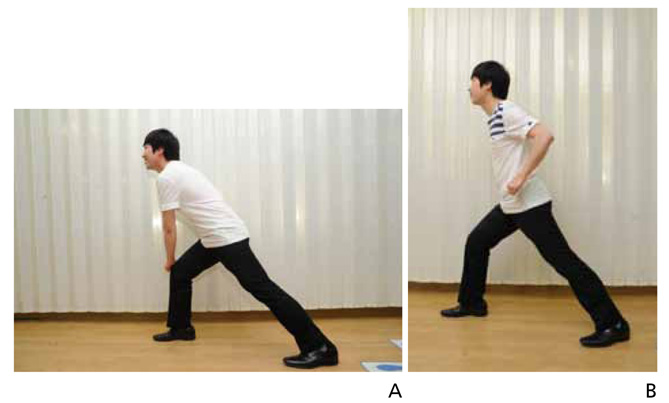
Figure 6 Lawnmower exercise done by beginning with the patient's trunk flexed and rotated to the contralateral side with the affected hand on the contralateral knee (A), and they are instructed to extend the trunk and rotate to the affected side with scapular retraction (B). Informed consent was received from the subject.
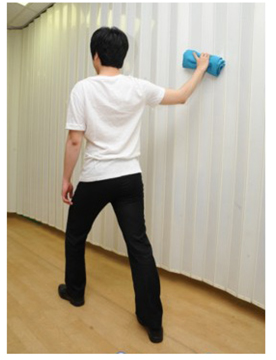
Figure 7 Wall wash exercise is a closed kinetic chain exercise. Standing by the wall with the unaffected side foot on the front and the affected side foot on the back, the patient touch the wall with a towel in the hand, and draws a big circle in forward direction.
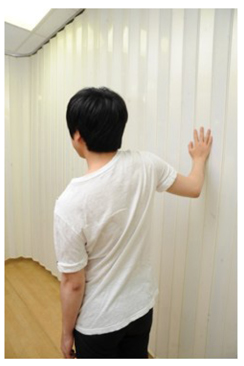
Figure 8 Scapular clock is a closed kinetic chain exercise. Standing one step away from the wall, the patient put the hand on the wall (with shoulder abducted less than 90 degrees) and slowly moves the shoulder in four directions; upward, downward, forward, and backward.

Figure 9 (A) A large calcification is shown in the supraspinatus tendon. (B) The needle tip is placed at the calcium deposit and small amount of normal saline & lidocaine mixture is repeatedly injected and aspirated back and forth, mechanically breaking the calcium mass.
Cited by 1 articles
-
Diagnosis and non-operative treatment of shoulder pain
Shi-Uk Lee
J Korean Med Assoc. 2019;62(12):629-635. doi: 10.5124/jkma.2019.62.12.629.
Reference
-
1. Jain TK, Sharma NK. The effectiveness of physiotherapeutic interventions in treatment of frozen shoulder/adhesive capsulitis: a systematic review. J Back Musculoskelet Rehabil. 2013; 11. 27. [Epub]. http://dx.doi.org/10.3233/BMR-130443.
Article2. Russell S, Jariwala A, Conlon R, Selfe J, Richards J, Walton M. A blinded, randomized, controlled trial assessing conservative management strategies for frozen shoulder. J Shoulder Elbow Surg. 2014; 23:500–507.
Article3. Yoon SH, Lee HY, Lee HJ, Kwack KS. Optimal dose of intra-articular corticosteroids for adhesive capsulitis: a randomized, triple-blind, placebo-controlled trial. Am J Sports Med. 2013; 41:1133–1139.
Article4. Carette S, Moffet H, Tardif J, Bessette L, Morin F, Fremont P, Bykerk V, Thorne C, Bell M, Bensen W, Blanchette C. Intraarticular corticosteroids, supervised physiotherapy, or a combination of the two in the treatment of adhesive capsulitis of the shoulder: a placebo-controlled trial. Arthritis Rheum. 2003; 48:829–838.
Article5. Buchbinder R, Green S, Youd JM, Johnston RV, Cumpston M. Arthrographic distension for adhesive capsulitis (frozen shoulder). Cochrane Database Syst Rev. 2008; (1):CD007005.
Article6. Kim K, Lee KJ, Kim HC, Lee KJ, Kim DK, Chung SG. Capsule preservation improves short-term outcome of hydraulic distension in painful stiff shoulder. J Orthop Res. 2011; 29:1688–1694.
Article7. Vastamaki H, Kettunen J, Vastamaki M. The natural history of idiopathic frozen shoulder: a 2- to 27-year followup study. Clin Orthop Relat Res. 2012; 470:1133–1143.
Article8. Kibler WB, McMullen J, Uhl T. Shoulder rehabilitation strategies, guidelines, and practice. Orthop Clin North Am. 2001; 32:527–538.
Article9. Escamilla RF, Hooks TR, Wilk KE. Optimal management of shoulder impingement syndrome. Open Access J Sports Med. 2014; 5:13–24.
Article10. Kibler WB, Sciascia AD, Uhl TL, Tambay N, Cunningham T. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. Am J Sports Med. 2008; 36:1789–1798.
Article11. Han TR, Bang MS, Chung SG. Rehabilitation medicine. 5th ed. Seoul: Koonja Publishing;2014.12. Re LP Jr, Karzel RP. Management of rotator cuff calcifications. Orthop Clin North Am. 1993; 24:125–132.
Article13. De Witte PB, Selten JW, Navas A, Nagels J, Visser CP, Nelissen RG, Reijnierse M. Calcific tendinitis of the rotator cuff: a randomized controlled trial of ultrasound-guided needling and lavage versus subacromial corticosteroids. Am J Sports Med. 2013; 41:1665–1673.14. Gatt DL, Charalambous CP. Ultrasound-guided barbotage for calcific tendonitis of the shoulder: a systematic review including 908 patients. Arthroscopy. 2014; 05. 09. [Epub]. http://dx.doi.org/10.1016/j.arthro.2014.03.013.
Article15. Pan PJ, Chou CL, Chiou HJ, Ma HL, Lee HC, Chan RC. Extracorporeal shock wave therapy for chronic calcific tendinitis of the shoulders: a functional and sonographic study. Arch Phys Med Rehabil. 2003; 84:988–993.
Article16. Peters J, Luboldt W, Schwarz W, Jacobi V, Herzog C, Vogl TJ. Extracorporeal shock wave therapy in calcific tendinitis of the shoulder. Skeletal Radiol. 2004; 33:712–718.
Article17. Shin SI, Song KW, Lee JY, Lee SY, Kim GR, Kim HC, Choi DE. Extracorporeal shock wave therapy for calcific tendinitis of the shoulder. J Korean Orthop Assoc. 2006; 41:865–870.
Article18. Huisstede BM, Gebremariam L, van der Sande R, Hay EM, Koes BW. Evidence for effectiveness of Extracorporal Shock-Wave Therapy (ESWT) to treat calcific and non-calcific rotator cuff tendinosis: a systematic review. Man Ther. 2011; 16:419–433.
Article19. Mouzopoulos G, Stamatakos M, Mouzopoulos D, Tzurbakis M. Extracorporeal shock wave treatment for shoulder calcific tendonitis: a systematic review. Skeletal Radiol. 2007; 36:803–811.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Most Common Shoulder Disorders
- The Management of Shoulder Pain in the Elderly: Focusing on Clinical Characteristics and Conservative Treatment
- Pulsed Radiofrequency Lesioning of the Axillary and Suprascapular Nerve in Calcific Tendinitis
- Treatment of Pain Around the Shoulder Joint
- Treatment Strategy for Frozen Shoulder
